The Meanings of Water: Socio-Cultural Perceptions of Solar Disinfected (SODIS) Drinking Water in Bolivia and Implications for its Uptake

 ,
, {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site
2.2. Data Collection
2.3. Data Analysis
2.4. Ethics
3. Results
3.1. Local Classification of Child Diarrhoea
3.2. Perceptions of Risks Associated with Drinking Water
- Moderator:
- ‘Have you ever seen these “bugs”?’
- Respondent 1:
- ‘We have not seen them, only the people from BoliviaWET have told us there are bugs. We have not seen them with our own eyes. If we saw them, they would disgust us, but if we don’t see them, we drink the water as if there were just nothing in there.’
- Respondent 2:
- ‘If we saw the bugs, we would not drink the water. We would appreciate if they would just show us. We could believe it if we saw what type of “bugs” they are talking about.’
- Moderator:
- ‘Don’t you trust them then?’
- Respondent 2:
- ‘Yes, yes, we do.’
- Moderator:
- ‘But you want to see them in order to believe it?’
- Respondent 1:
- ‘If we don’t see, we don’t believe. We ask ourselves, will it always be true? But we see our water is clean.’
- Moderator:
- ‘When you drink a certain type of water, can you get diarrhoea or fall ill?’
- Respondent 2:
- ‘No, our stomachs are already used to it […] Maybe we get diarrhoea from the water from another source.’
- Respondent 3:
- ‘We don’t know where the diarrhoea comes from, because every day we drink this water, some of us since we were born.’
- Moderator:
- ‘And doesn’t it affect you?’
- Respondent 3:
- ‘We don’t know from what we get ill from. If we drank this water and fell ill shortly after, it could be. However, this is not the case. We drink this water every day.’
3.3. Perceived Efficacy of the SODIS HWT Method
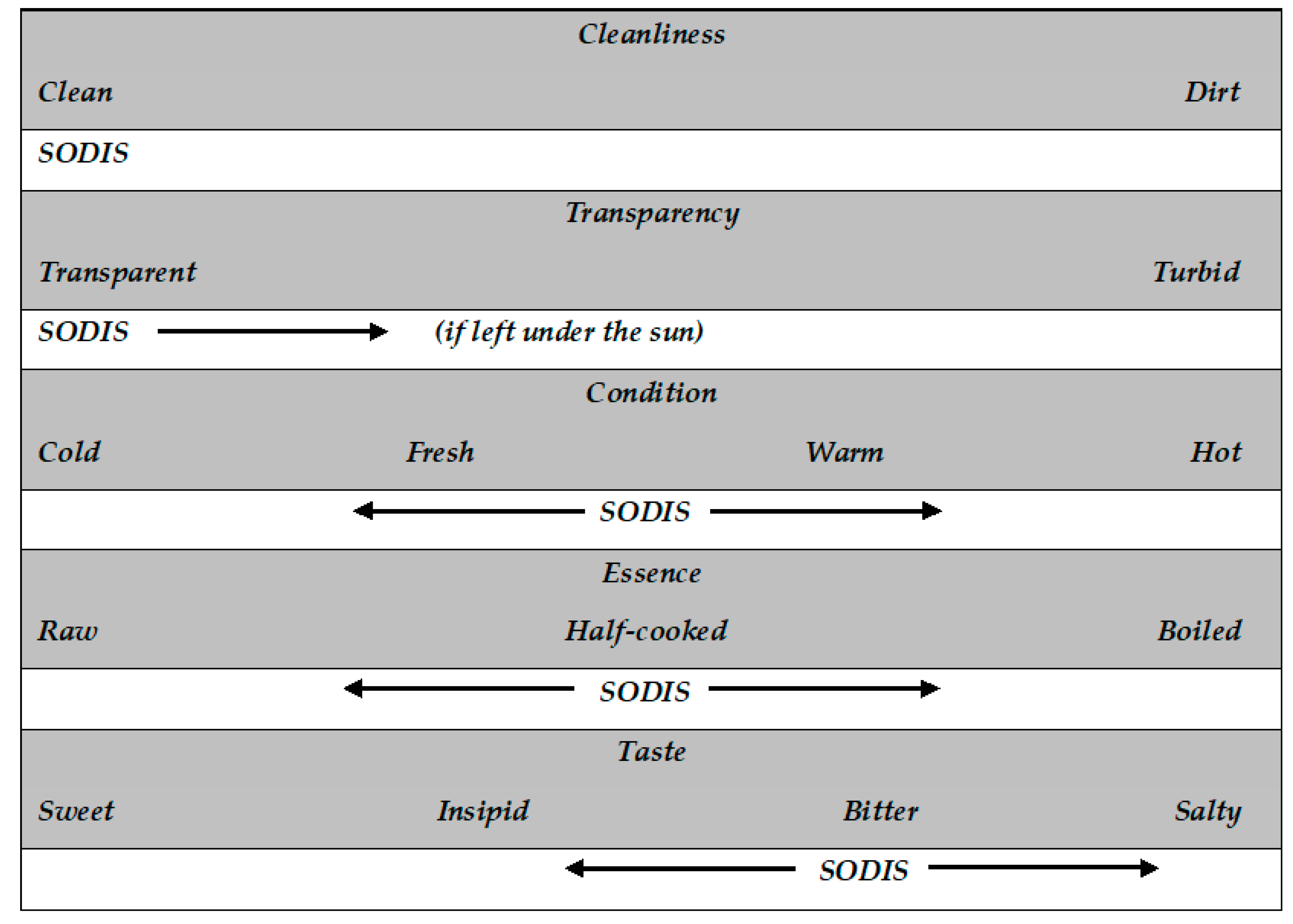
3.4. Local Classification of Drinking Water
- a-
- ‘Boiled’ like boiled water, because ‘the sun boiled the water’,
- b-
- ‘Boiled’ but to a lesser degree than boiled water,
- c-
- Neither ‘raw’ nor ‘boiled’: ‘it looks like “raw” water, but it is not because it is also sort of half-boiled. It has been cooked by the sun; thus, it doesn’t appear natural anymore’,
- d-
- ‘Badly boiled’ (closer to ‘raw’ water) and, therefore, potentially harmful: ‘SODIS water is always “raw” as it is only warmed in the sun […]. Whereas boiling makes the water well-cooked, what does the sun do?’
3.5. The Taste of SODIS Water as a Barrier for its Uptake
4. Discussion
4.1. SODIS Water Within the Local Interpretation of the ‘Hot and Cold’ Theory
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McGuigan, K.G.; Joyce, T.M.; Conroy, R.M.; Gillespie, J.B.; Elmore-Meegan, M. Solar disinfection of drinking water contained in transparent plastic bottles: Characterizing the bacterial inactivation process. J. Appl. Microbiol. 1998, 84, 1138–1148. [Google Scholar] [CrossRef] [Green Version]
- Boyle, M.; Sichel, C.; Fernandez-Ibanez, P.; Arias-Quiroz, G.B.; Iriarte-Puna, M.; Mercado, A.; Ubomba-Jaswa, E.; McGuigan, K.G. Bactericidal Effect of Solar Water Disinfection under Real Sunlight Conditions. Appl. Environ. Microbiol. 2008, 74, 2997–3001. [Google Scholar] [CrossRef] [Green Version]
- DeJung, S.; Fuentes, I.; Almanza, G.; Jarro, R.; Navarro, L.; Arias, G.; Urquieta, E.; Torrico, A.; Fenandez, W.; Iriarte, M.; et al. Effect of solar water disinfection (SODIS) on model microorganisms under improved and field SODIS conditions. J. Water Supply Res. Technol. 2007, 56, 245–256. [Google Scholar] [CrossRef] [Green Version]
- McGuigan, K.G.; Conroy, R.M.; Mosler, H.-J.; Du Preez, M.; Ubomba-Jaswa, E.; Fernandez-Ibañez, P. Solar water disinfection (SODIS): A review from bench-top to roof-top. J. Hazard. Mater. 2012, 235, 29–46. [Google Scholar] [CrossRef] [PubMed]
- Meierhofer, R.; Landolt, G. Factors supporting the sustained use of solar water disinfection—Experiences from a global promotion and dissemination programme. Desalination 2009, 248, 144–151. [Google Scholar] [CrossRef]
- Moser, S.; Mosler, H.-J. Differences in influence patterns between groups predicting the adoption of a solar disinfection technology for drinking water in Bolivia. Soc. Sci. Med. 2008, 67, 497–504. [Google Scholar] [CrossRef]
- Tamas, A.; Mosler, H.-J. Why Do People Stop Treating Contaminated Drinking Water with Solar Water Disinfection (SODIS)? Health Educ. Behav. 2011, 38, 357–366. [Google Scholar] [CrossRef]
- World Health Organization. Drinking Water Equity, Safety and Sustainability: Thematic Report on Drinking Water; WHO: New York, NY, USA; UNICEF: New York, NY, USA, 2011; p. 64. [Google Scholar]
- Rainey, R.C.; Harding, A.K. Acceptability of solar disinfection of drinking water treatment in Kathmandu Valley, Nepal. Int. J. Environ. Health Res. 2005, 15, 361–372. [Google Scholar] [CrossRef]
- Arnold, B.; Arana, B.; Mäusezahl, D.; Hubbard, A.; Colford, J.M. Evaluation of a pre-existing, 3-year household water treatment and handwashing intervention in rural Guatemala. Int. J. Epidemiol. 2009, 38, 1651–1661. [Google Scholar] [CrossRef]
- Du Preez, M.; McGuigan, K.G.; Conroy, R.M. Solar Disinfection of Drinking Water In the Prevention of Dysentery in South African Children Aged under 5 Years: The Role of Participant Motivation. Environ. Sci. Technol. 2010, 44, 8744–8749. [Google Scholar] [CrossRef]
- Hartinger, S.M.; Lanata, C.F.; Hattendorf, J.; Verastegui, H.I.; Gil, A.; Wolf, J.; Mäusezahl, D. Improving household air, drinking water and hygiene in rural Peru: A community-randomized-controlled trial of an integrated environmental home-based intervention package to improve child health. Int. J. Epidemiol. 2016, 45, 2089–2099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mäusezahl, D.; Christen, A.; Pacheco, G.D.; Tellez, F.A.; Iriarte, M.; Zapata, M.E.; Cevallos, M.; Hattendorf, J.; Cattaneo, M.D.; Arnold, B.; et al. Solar Drinking Water Disinfection (SODIS) to Reduce Childhood Diarrhoea in Rural Bolivia: A Cluster-Randomized, Controlled Trial. PLoS Med. 2009, 6, e1000125. [Google Scholar] [CrossRef] [PubMed]
- Islam, A.; Azad, A.K.; Akber, A.; Rahman, M.; Sadhu, I. Effectiveness of solar disinfection (SODIS) in rural coastal Bangladesh. J. Water Heal. 2015, 13, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Altherr, A.M.; Mosler, H.J.; Tobias, R.; Butera, F. Attitudinal and relational factors predicting the use of solar water disinfection: A field study in Nicaragua. Health Educ. Behav. 2008, 35, 207–220. [Google Scholar] [CrossRef] [Green Version]
- Christen, A.; Pacheco, G.D.; Hattendorf, J.; Arnold, B.F.; Cevallos, M.; Indergand, S.; Colford, J.M.; Mäusezahl, D. Factors associated with compliance among users of solar water disinfection in rural Bolivia. BMC Public Health 2011, 11, 210. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, S.M.; Mosler, H.-J. Persuasion factors influencing the decision to use sustainable household water treatment. Int. J. Environ. Health Res. 2010, 20, 61–79. [Google Scholar] [CrossRef]
- Foster, G.M. Disease Etiologies in Non-Western Medical Systems. Am. Anthropol. 1976, 78, 773–782. [Google Scholar] [CrossRef]
- Kleinman, A.; Gale, J.L. Patients treated by physicians and folk healers: A comparative outcome study in Taiwan. Cult. Med. Psychiatry 1982, 6, 405–423. [Google Scholar] [CrossRef]
- Sikkink, L. New Cures, Old Medicines: Women and the Commercialization of Traditional Medicine in Bolivia; Wadsworth Publishing Company: Belmont, CA, USA, 2009. [Google Scholar]
- Gutiérrez, M.E. Ambivalencias elementales. Representaciones ameríndias. Quad. l’Inst. Català d’Antropol. 2009, 25, 141–160. [Google Scholar]
- Messer, E. Hot-cold classification: Theoretical and practical implications of a Mexican study. Soc. Sci. Med. 1981, 15, 133–145. [Google Scholar] [CrossRef]
- Weiss, M.G. Cultural models of diarrheal illness: Conceptual framework and review. Soc. Sci. Med. 1988, 27, 5–16. [Google Scholar] [CrossRef]
- Ahmed, M.J.; Van Veen, A.G. A sociological approach to a dietary survey and food habit study in an Andean community. Trop. Geogr. Med. 1968, 20, 88–100. [Google Scholar] [PubMed]
- Mazess, R.B. Hot-cold food beliefs among Andean peasants. J. Am. Diet. Assoc. 1968, 53, 109–113. [Google Scholar]
- Pacheco, G.D.; Christen, A.; Arnold, B.; Hattendorf, J.; Colford, J.M.; Smith, T.A.; Mäusezahl, D. Reporting Diarrhoea through a Vernacular Term in Quechua-speaking Settings of Rural Bolivia. J. Health Popul. Nutr. 2011, 29, 552–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobbins, M. Home-Based Drinking Water Purification through Sunlight: From Promotion to Health Effectiveness; University of Basel: Basel, Switzerland, 2004. [Google Scholar]
- Bryman, A. Social Research Methods; Oxford University Press: Oxford, UK, 2008. [Google Scholar]
- Dawson, S.; Manderson, L.; Tallo, V.L. A Manual for the Use of Focus Groups; International Nutrition Foundation for Developing Countries: Boston, MA, USA, 1993. [Google Scholar]
- Currier, R.L. The Hot-Cold Syndrome and Symbolic Balance in Mexican and Spanish-American Folk Medicine. Ethnology 1966, 5, 251–263. [Google Scholar] [CrossRef]
- Logan, M.H. New lines of inquiry on the illness of Susto. Med. Anthropol. 1993, 15, 189–200. [Google Scholar] [CrossRef]
- Rubel, A.J.; O’Nell, C.W.; Collado-Ardón, R. Susto, a Folk Illness; University of California Press: Berkeley, CA, USA, 1985. [Google Scholar]
- Moser, S.; Heri, S.; Mosler, H.J. Determinants of the Diffusion of SODIS: A Quantitative Field Study in Bolivia; Summary Report; EAWAG: Duebendorf, Switzerland, 2005. [Google Scholar]
- Pacheco, G.D.; Swiss Tropical and Public Health Institute, Basel, Switzerland. Personal Communication, 2009.
- Antropología Y Desarrollo. Discursos, Prácticas Y Actores; Pérez, B., Ed.; La Catarata: Madrid, Spain, 2012. [Google Scholar]
- Bourdieu, P. Raisons Pratiques. Sur La Théorie De L’action; Éditions du Seuil: Paris, France, 1994. [Google Scholar]
- Heri, S.; Mosler, H.J. Factors affecting the diffusion of solar water disinfection: A field study in Bolivia. Health Educ. Behav. 2008, 35, 541–560. [Google Scholar] [CrossRef]
- Halperin, M.; Paz-Soldán, V.A.; Quispe, V.; Paxton, A.; Gilman, R.H. Student Column: Sustain Ability of Solar Disinfection to Provide Safe Drinking Water in Rural Peru. Public Health Rep. 2011, 126, 762–768. [Google Scholar] [CrossRef] [Green Version]
- Hartinger, S.M.; Lanata, C.F.; Gil, A.I.; Hattendorf, J.; Verastegui, H.; Mäusezahl, D. Combining Interventions: Improved Chimney Stoves, Kitchen Sinks and Solar Disinfection of Drinking Water and Kitchen Clothes to Improve Home Hygiene In Rural Peru. F. Actions Sci. Rep. 2012, 6. Available online: https://journals.openedition.org/factsreports/1627 (accessed on 4 February 2019).
- Roma, E.; Bond, T.; Jeffrey, P. Factors involved in sustained use of point-of-use water disinfection methods: A field study from Flores Island, Indonesia. J. Water Health 2014, 12, 573–583. [Google Scholar] [CrossRef]
- Kaplan, M. Lonely drinking fountains and comforting coolers: Paradoxes of water value and ironies of water use. Cult. Anthropol. 2011, 26, 514–541. [Google Scholar] [CrossRef] [PubMed]
- de França, M.D. Factors influencing public perception of drinking water quality. Water Policy 2010, 12, 1–19. [Google Scholar] [CrossRef]
- Jardine, C.; Gibson, N.; Hrudey, S. Detection of odour and health risk perception of drinking water. Water Sci. Technol. 1999, 40, 91–98. [Google Scholar] [CrossRef]
- Yasar, A.; Khan, N.Y.; Batool, A.; Tabinda, A.B.; Mehmood, R.; Iqbal, A. Women Perception of Water Quality and its Impacts on Health in Gangapur, Pakistan. Pak. J. Nutr. 2011, 10, 702–706. [Google Scholar] [CrossRef] [Green Version]
- Mosler, H.-J. A systematic approach to behavior change interventions for the water and sanitation sector in developing countries: A conceptual model, a review, and a guideline. Int. J. Environ. Health Res. 2012, 22, 431–449. [Google Scholar] [CrossRef]
- Tamás, A.; Tobias, R.; Mosler, H.-J. Promotion of Solar Water Disinfection: Comparing the Effectiveness of Different Strategies in a Longitudinal Field Study in Bolivia. Health Commun. 2009, 24, 711–722. [Google Scholar] [CrossRef]
- Mosler, H.-J.; Kraemer, S.; Johnston, R. Achieving long-term use of solar water disinfection in Zimbabwe. Public Health 2013, 127, 92–98. [Google Scholar] [CrossRef]
- Heierli, U. Marketing safe water systems. In Why is it so Hard to Get Safe Water to the Poor- and so Profitable to Sell it to the Rich; Swiss Agency for Development and Cooperation (SDC): Bern, Switzerland, 2008. [Google Scholar]
- Arnold, B.F.; Colford, J.M. Treating water with chlorine at point-of-use to improve water quality and reduce child diarrhea in developing countries: A systematic review and meta-analysis. Am. J. Trop. Med. Hyg. 2007, 76, 354–364. [Google Scholar] [CrossRef] [Green Version]
- Kayaga, S.; Reed, B. Emergency Treatment of Drinking-Water at the Point of Use; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Conroy, R.M.; Elmore-Meegan, M.; Joyce, T.; McGuigan, K.G.; Barnes, J. Solar disinfection of drinking water and diarrhoea in Maasai children: A controlled field trial. Lancet 1996, 348, 1695–1697. [Google Scholar] [CrossRef]
- Conroy, R.M.; Meegan, M.E.; Joyce, T.; McGuigan, K.; Barnes, J. Solar disinfection of water reduces diarrhoeal disease: An update. Arch. Dis. Child. 1999, 81, 337–338. [Google Scholar] [CrossRef] [Green Version]
- Foster, G.M. The validating role of humoral theory in traditional Spanish? American therapeutics. Am. Ethnol. 1988, 15, 120–135. [Google Scholar] [CrossRef]
- García, J.A. Dieta y salud en época Clásica. Baética Estud. Arte Geogr. Hist. 2010, 32, 157–176. [Google Scholar]
- Lain, P.E. La Medicina Hipocrática; Alianza: Madrid, Spain, 1983. [Google Scholar]
- Tilley, E.; Strande, L.; Lüthi, C.; Mosler, H.-J.; Udert, K.M.; Gebauer, H.; Hering, J.G. Looking beyond Technology: An Integrated Approach to Water, Sanitation and Hygiene in Low Income Countries. Environ. Sci. Technol. 2014, 48, 9965–9970. [Google Scholar] [CrossRef] [PubMed]
- Béhague, M.P.; Gonçalves, H.; Victora, C.G. Anthropology and Epidemiology: Learning epistemological lessons through a collaborative venture. Ciência Saúde Coletiva 2008, 13, 1701–1710. [Google Scholar] [CrossRef] [Green Version]
- Hadorn, G.H.; Hoffmann-Riem, H.; Biber-Klemm, S.; Grossenbacher-Mansuy, W.; Joye, D.; Pohl, C.; Wiesmann, U.; Zemp, E. Handbook of Transdisciplinary Research; Springer: Dordrecht, The Netherlands, 2008. [Google Scholar]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuño Martínez, N.; Muela Ribera, J.; Hausmann-Muela, S.; Cevallos, M.; Hartinger, S.M.; Christen, A.; Mäusezahl, D. The Meanings of Water: Socio-Cultural Perceptions of Solar Disinfected (SODIS) Drinking Water in Bolivia and Implications for its Uptake. Water 2020, 12, 442. https://doi.org/10.3390/w12020442
Nuño Martínez N, Muela Ribera J, Hausmann-Muela S, Cevallos M, Hartinger SM, Christen A, Mäusezahl D. The Meanings of Water: Socio-Cultural Perceptions of Solar Disinfected (SODIS) Drinking Water in Bolivia and Implications for its Uptake. Water. 2020; 12(2):442. https://doi.org/10.3390/w12020442
Chicago/Turabian StyleNuño Martínez, Néstor, Joan Muela Ribera, Susanna Hausmann-Muela, Myriam Cevallos, Stella María Hartinger, Andri Christen, and Daniel Mäusezahl. 2020. "The Meanings of Water: Socio-Cultural Perceptions of Solar Disinfected (SODIS) Drinking Water in Bolivia and Implications for its Uptake" Water 12, no. 2: 442. https://doi.org/10.3390/w12020442