Human Health Risks Associated with Recreational Waters: Preliminary Approach of Integrating Quantitative Microbial Risk Assessment with Microbial Source Tracking

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. E. coli Monitoring Data
2.3. Reference Pathogens
2.4. Exposure Variables and Dose Calculations
- is the dose of reference pathogen (# oocysts, viral particles, or CFU)
- S is the specified source
- is the concentration of the bacterial indicator E. coli in the waterbody (
- is the fraction of the total amount of indicator bacteria from the specific source
- is the density of the bacterial indicator, E. coli, to the wet mass of the nonhuman waste or human waste (
- is the density of the reference pathogen in the fecal waste (wet mass) or in sewage (
- is the prevalence of infection for the reference pathogen and source
- is the infectious potential of the reference pathogen in humans
- V is the water volume ingested (mL)
2.5. Calculating Total Probability of Illness for a Mixture of Fecal Sources
2.6. Characterizing Human Health Risk
3. Results
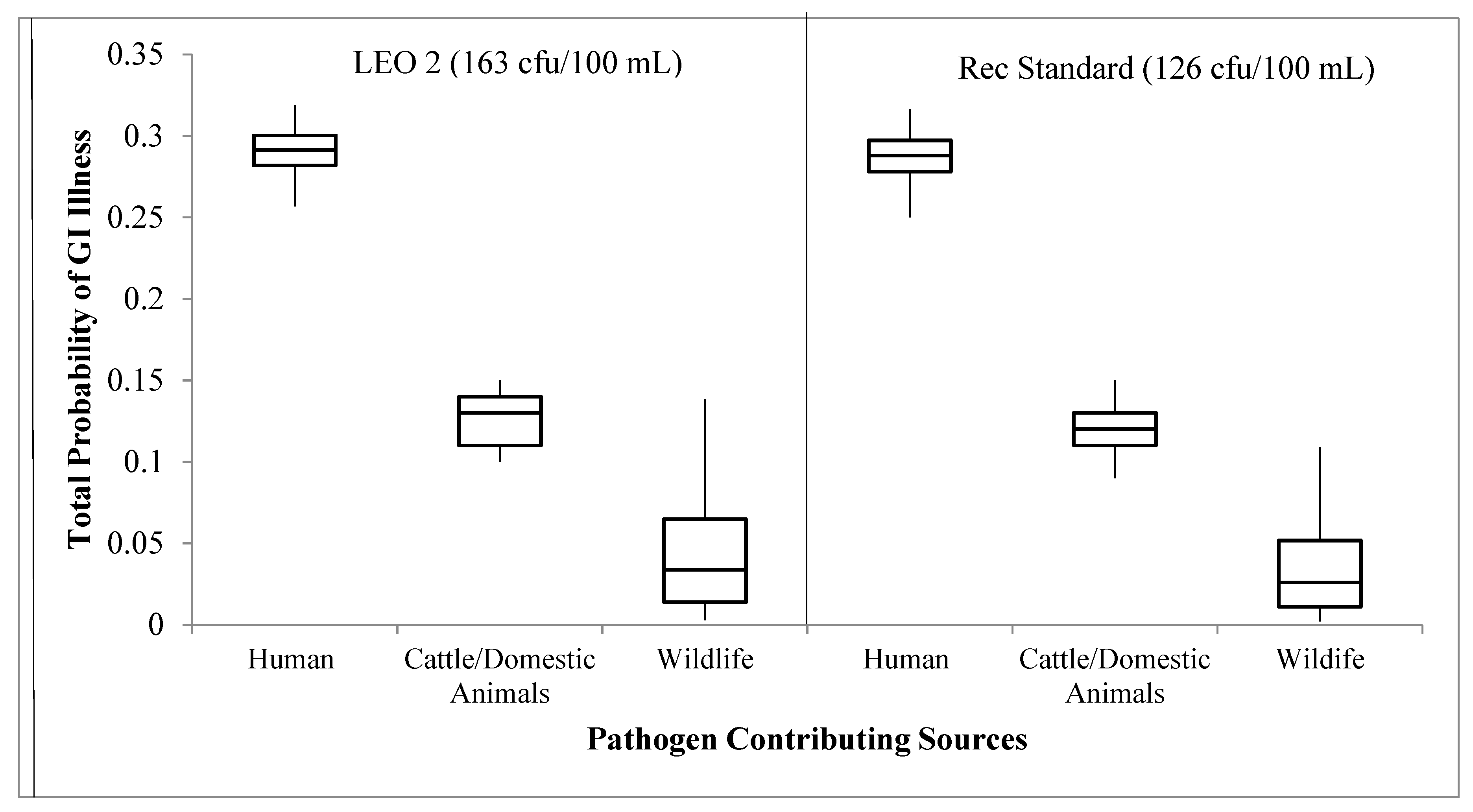
3.1. Scenario 1: Each Source Contributing 100%
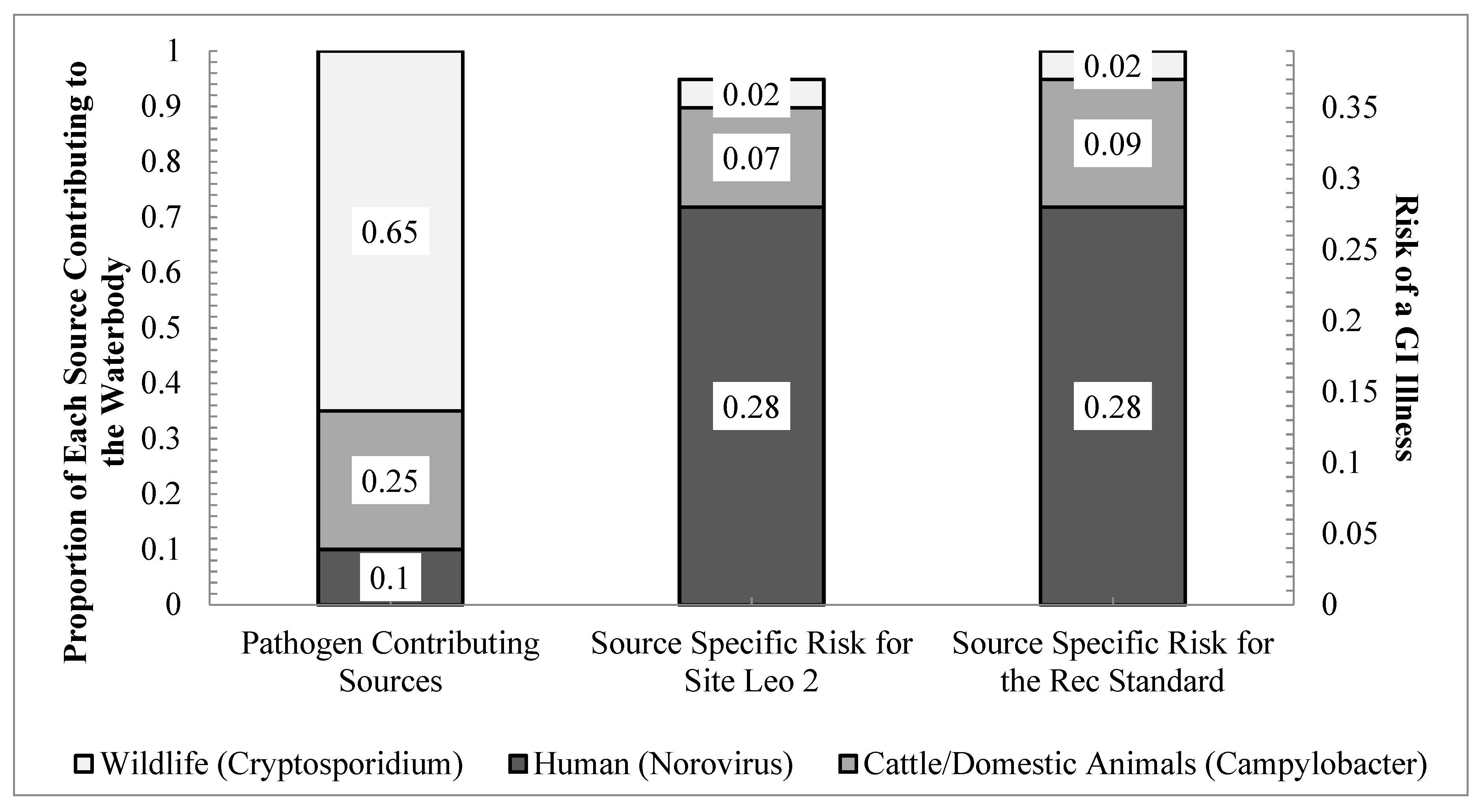
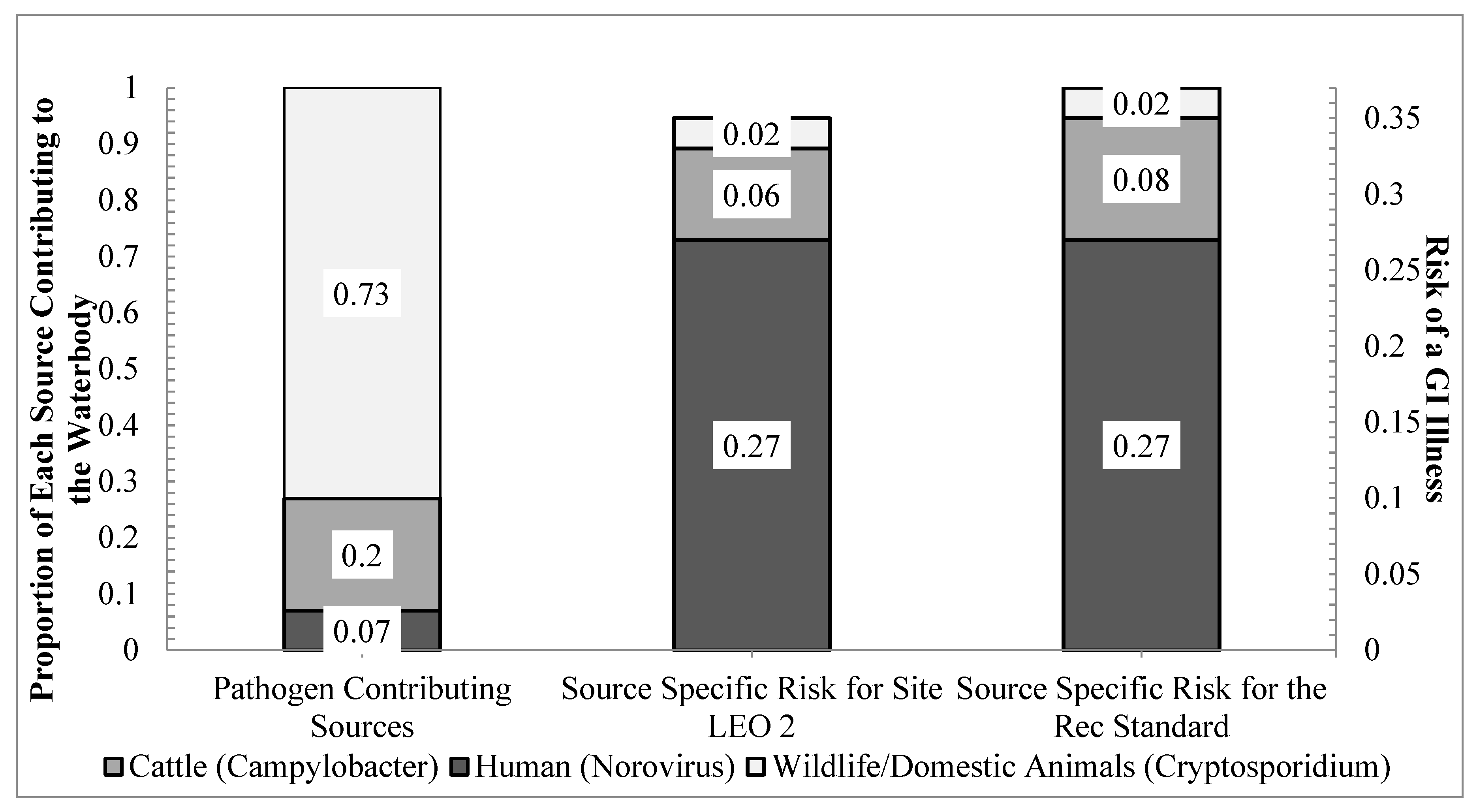
3.2. Scenarios 2 and 3: Source Contributions Based on MST and Modified MST Results
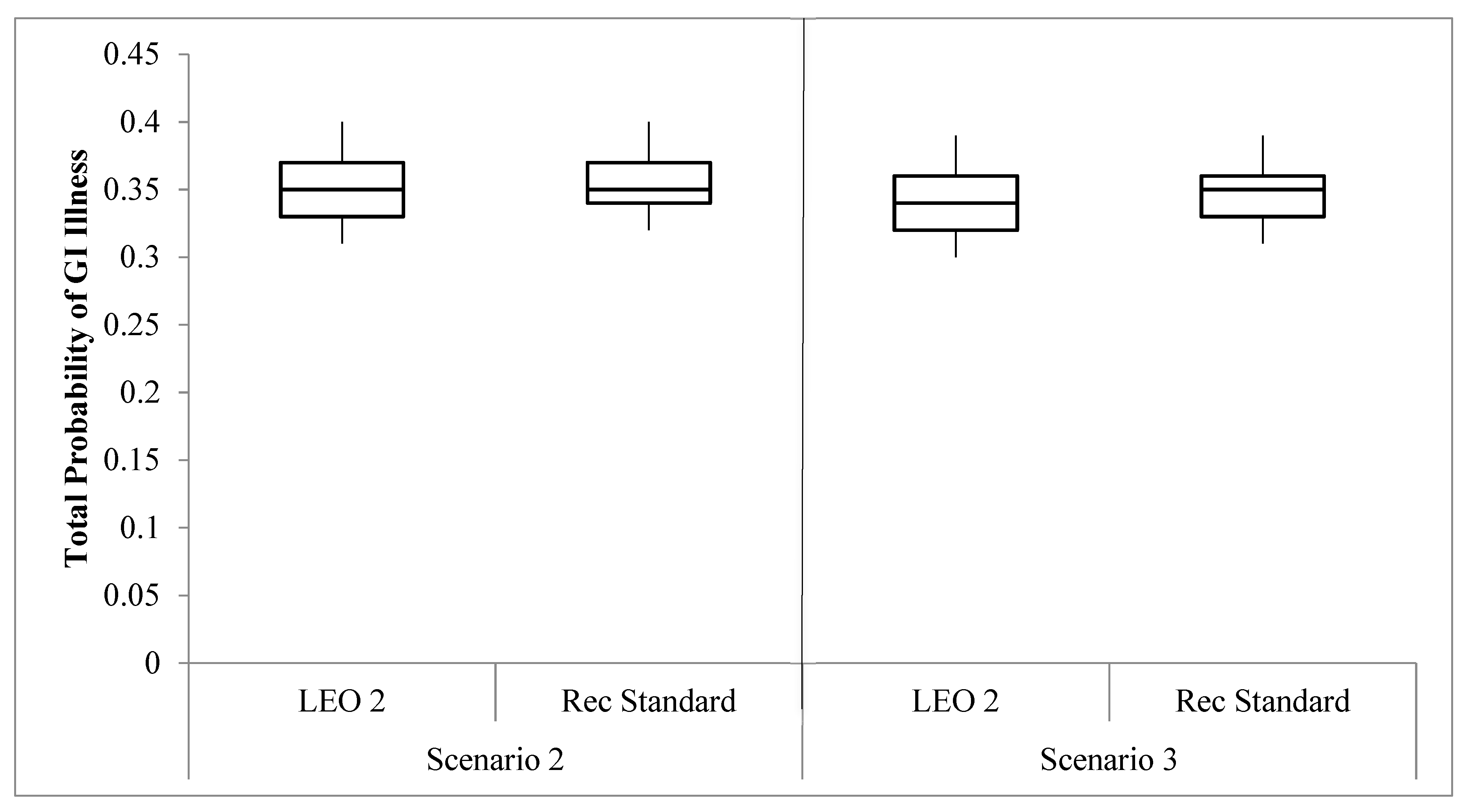
3.3. Comparison of the Total Probability of Illness Risks
3.4. Sensitivity Analysis of the Uncertainty in Simulations
4. Discussion
4.1. Scenario Assessment and Risks of a GI Illness
4.2. Source Contributing the Greatest Human Health Risk
4.3. Study Limitations
4.4. QMRA Applicability for the Future
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schoen, M.E.; Ashbolt, N.J. Assessing pathogen risk to swimmers at non-sewage impacted recreational beaches. Environ. Sci. Technol. 2010, 44, 2286–2291. [Google Scholar] [CrossRef] [PubMed]
- Soller, J.A.; Bartrand, T.; Ashbolt, N.J.; Ravenscroft, J.; Wade, T.J. Estimating the primary etiologic agents in recreational freshwaters impacted by human sources of faecal contamination. Water Res. 2010, 44, 4736–4747. [Google Scholar] [CrossRef] [PubMed]
- Soller, J.A.; Schoen, M.E.; Bartrand, T.; Ravenscroft, J.E.; Ashbolt, N.J. Estimated human health risks from exposure to recreational waters impacted by human and non-human sources of faecal contamination. Water Res. 2010, 44, 4674–4691. [Google Scholar] [CrossRef]
- Soller, J.A.; Schoen, M.E.; Varghese, A.; Ichida, A.M.; Boehm, A.B.; Eftim, S.; Ashbolt, N.J.; Ravenscroft, J.E. Human health risk implications of multiple sources of faecal indicator bacteria in a recreational waterbody. Water Res. 2014, 66, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Soller, J.; Bartrand, T.; Ravenscroft, J.; Molina, M.; Whelan, G.; Schoen, M.; Ashbolt, N. Estimated human health risks from recreational exposures to stormwater runoff containing animal faecal material. Environ. Model. Softw. 2015, 72, 21–32. [Google Scholar] [CrossRef]
- Di Giovanni, G.D.; Gentry, T.J.; Martin, E.; Gregory, L.; Wagner, K. Support Analytical Infrastructure and Further Development of a Statewide Bacterial Source Tracking Library Report TR-448; Texas Water Resources Institute: College Station, TX, USA, 2013. [Google Scholar]
- Arnone, R.D.; Walling, J.P. Waterborne pathogens in urban watersheds. J. Water Health 2007, 4, 149–162. [Google Scholar] [CrossRef]
- Pandey, P.K.; Kass, P.H.; Soupir, M.L.; Biswas, S.; Singh, V.P. Contamination of water resources by pathogenic bacteria. AMB Express 2014, 4, 1–16. [Google Scholar] [CrossRef] [Green Version]
- USEPA. Recreational Water Quality Criteria Report 820-F-12-058; U.S. Environmental Protection Agency Office of Water: Washington, DC, USA, 2012. [Google Scholar]
- USEPA. Quantitative Microbial Risk Assessment to Estimate Illness in Freshwater Impacted by Agricultural Animal Sources of Fecal Contamination Report EPA 822-R-10-005; U.S. Environmental Protection Agency Office of Water: Washington, DC, USA, 2010. [Google Scholar]
- Schijven, J.F.; de Roda Husman, A.M. Applications of Quantitative Microbial Source Tracking (QMST) and Quantitative Microbial Risk Assessment (QMRA). In Microbial Source Tracking: Methods, Applications, and Case Studies; Hagedorn, C., Blanch, A.R., Harwood, V.J., Eds.; Springer: New York, NY, USA, 2011; pp. 559–583. [Google Scholar]
- Gregory, L.; Casarez, E.; Truesdale, J.; Di Giovanni, G.; Owen, T.; Wolfe, J. Bacterial Source Tracking to Support. the Development and Implementation of Watershed Protection Plans for the Lampasas and Leon Rivers TR-442; Texas Water Resources Institute: College Station, TX, USA, 2013. [Google Scholar]
- Bragg, J.; Vargas, M.; Dulcay, M. Watershed Protection Plan for the Leon River below Proctor Lake and above Belton Lake. 2011. Available online: http://leonriver.tamu.edu/media/1110/final-leon-wpp.pdf (accessed on 16 July 2016).
- Versalovic, J.; Schneider, M.; De Bruijn, F.J.; Lupski, J.R. Genomic fingerprinting of bacteria using repetitive sequence-based polymerase chain reaction. Meth. Mol. Cell Biol. 1994, 5, 25–40. [Google Scholar]
- Casarez, E.A.; Pillai, S.D.; Mott, J.B.; Vargas, M.; Dean, K.E.; Di Giovanni, G.D. Direct comparison of four bacterial source tracking methods and use of composite data sets. J. Appl. Microbiol. 2007, 103, 350–364. [Google Scholar] [CrossRef]
- Casarez, E.A.; Pillai, S.D.; Di Giovanni, G.D. Genotype diversity of Escherichia coli isolates in natural waters determined by PFGE and ERIC-PCR. Water Res. 2007, 41, 3643–3648. [Google Scholar] [CrossRef]
- Schoen, M.E.; Soller, J.A.; Ashbolt, N.J. Evaluating the importance of faecal sources in human-impacted waters. Water Res. 2011, 45, 2670–2680. [Google Scholar] [CrossRef] [PubMed]
- Van Abel, N.; Schoen, M.E.; Kissel, J.C.; Meschke, J.S. Comparison of risk predicted by multiple norovirus dose–response models and implications for quantitative microbial risk assessment. Risk Anal. 2016, 37, 245–264. [Google Scholar] [CrossRef] [PubMed]
- Carmena, D. Waterborne transmission of Cryptosporidium and Giardia: Detection, surveillance and implications for public health. In Current Research, Technology and Education Topics in Applied Microbiology and Microbial Biotechnology; Mendez-Vilas, A., Ed.; Formatex: Badajoz, Spain, 2010; Volume 1, pp. 3–14. [Google Scholar]
- Zahedi, A.; Paparini, A.; Jian, F.; Robertson, I.; Ryan, U. Public health significance of zoonotic Cryptosporidium species in wildlife: Critical insights into better drinking water management. Int. J. Parasitol. Parasites Wildl. 2016, 5, 88–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graczyk, T.K.; Majewska, A.C.; Schwab, K.J. The role of birds in dissemination of human waterborne enteropathogens. Trends. Parasitol. 2008, 24, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Dufour, A.P.; Evans, O.; Behymer, T.D.; Cantu, R. Water ingestion during swimming activities in a pool: A pilot study. J. Water Health 2006, 4, 425–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunger, N.; Haas, C.N. Quantitative microbial risk assessment for recreational exposure to water bodies in Philadelphia. Water Environ. Res. 2015, 87, 211–222. [Google Scholar] [CrossRef]
- Padia, R.; Karthikeyan, R.; Mukhtar, S.; Parker, I. Occurrence and fate of E. coli from various non-point sources in a subtropical watershed. J. Nat. & Environ. Sci 2012, 3, 9–18. [Google Scholar]
- Telesford-Checkley, J.M.; Mora, M.A.; Gentry, T.J.; McDonald, T.J.; Boellstorff, D.E. Impacts of heronries on water quality as evaluated through Escherichia coli and Fecal Sterol Analyses. Water Environ. Res. 2017, 89, 508–518. [Google Scholar] [CrossRef]
- Appelbee, A.J.; Thompson, R.A.; Olson, M.E. Giardia and Cryptosporidium in mammalian wildlife–current status and future needs. Trends Parasitol. 2005, 21, 370–376. [Google Scholar] [CrossRef]
- Thomas, J.L.; Pintar, K.D.; Wallis, P.M.; Neumann, N.F. Using host-specificity of Cryptosporidium to understand contaminant sources, seasonality, and human health risk in three watersheds of differing land-use. J. Environ. Prot. 2016, 7, 372–381. [Google Scholar] [CrossRef] [Green Version]
- Rosef, O.; Kapperud, G.; Lauwers, S.; Gondrosen, B. Serotyping of Campylobacter jejuni, Campylobacter coli and Campylobacter laridis from domestic and wild animals. Appl. Environ. Microbiol. 1985, 49, 1507–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, L.; Nielsen, E.M.; Engber, J.; On, S.L.W.; Dietz, H.H. Comparison of genotypes and serotypes of Campylobacter jejuni isolated from Danish wild mammals and birds and from broiler flocks and humans. Appl. Environ. Microbiol. 2001, 67, 3115–3121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, E.M.; Engberg, J.; Madsen, M. Distribution of serotypes of Campylobacter jejuni and C. coli from Danish patients, poultry, cattle and swine. FEMS Immunol. Med. Microbiol. 1997, 19, 47–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McBride, G.B.; Stott, R.; Miller, W.; Bambic, D.; Wuertz, S. Discharge-based QMRA for estimation of public health risks from exposure to stormwater-borne pathogens in recreational waters in the United States. Water Res. 2013, 47, 5282–5297. [Google Scholar] [CrossRef] [PubMed]
- Lindesmith, L.C.; Donaldson, E.F.; Baric, R.S. Norovirus GII. 4 strain antigenic variation. J. Virol. 2011, 85, 231–242. [Google Scholar] [CrossRef] [Green Version]
- Atwill, E.R.; Phillips, R.; Rulofson, F. Environmental loading rates of the waterborne pathogenic protozoa Cryptosporidium parvum in certain domestic and wildlife species in California. In Proceedings of the Vertebrate Pest Conference, Reno, NV, USA, 4–7 Macch 2002. [Google Scholar]
- Medema, G.J.; Teunis, P.F.M.; Havelaar, A.H.; Haas, C.N. Assessment of the dose-response relationship of Campylobacter jejuni. Int. J. Food Microbiol. 1996, 30, 101–111. [Google Scholar] [CrossRef]
- Teunis, P.F.; Moe, C.L.; Liu, P.; Miller, S.E.; Lindesmith, L.; Baric, R.S.; Le Pendu, J.; Calderon, R.L. Norwalk virus: How infectious is it? J. Med. Virol. 2008, 80, 1468–1476. [Google Scholar] [CrossRef]
- Teunis, P.F.M.; van den Brandhofl, W.; Nauta, M.; Wagenaar, J.; van den Kerkhof, H.; van Pelt, W. A reconsideration of the Campylobacter dose-response relation. Epidemiol. Infect. 2005, 133, 583–592. [Google Scholar] [CrossRef]
- USEPA. Economic Analysis for the Final Long Term 2 Enhanced Surface Water Treatment Rule Report 815-R-06-001; U.S. Environmental Protection Agency Office of Water: Washington, DC, USA, 2005. [Google Scholar]
- Soller, J.; Eftim, S.E.; Warren, I.; Nappier, S.P. Evaluation of microbiological risks associated with direct potable reuse. Microbi. Risk Anal. 2017, 5, 3–14. [Google Scholar] [CrossRef]
- Eisenberg, J.; Seto, E.Y.W.; Olivieri, A.W.; Spear, R.C. Quantifying water pathogen risk in an epidemiological framework. Risk Anal. 1996, 16, 549–563. [Google Scholar] [CrossRef]
- Ahmed, W.; Hamilton, K.A.; Lobos, A.; Hughes, B.; Staley, C.; Sadowsky, M.J.; Harwood, V.J. Quantitative microbial risk assessment of microbial source tracking markers in recreational water contaminated with fresh untreated and secondary treated sewage. Environ. Int. 2018, 117, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Pandey, P.K.; Soupir, M.L. Assessing the impacts of E. coli laden streambed sediment on E. coli loads over a range of flows and sediment characteristics. J. Am. Water Resour. Assoc. 2013, 49, 1261–1269. [Google Scholar] [CrossRef]
- Korajkic, A.; McMinn, B.R.; Harwood, V.J.; Shanks, O.C.; Fout, G.S.; Ashbolt, N.J. Differential decay of enterococci and Escherichia coli originating from two fecal pollution sources. Appl Environ. Microb 2013, 79, 2488–2492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerba, C.P.; Rose, J.B.; Haas, C.N. Sensitive populations: Who is at the greatest risk? Int. J. Food Microbiol. 1996, 30, 113–123. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Input Data | Comments | Distribution | Source |
|---|---|---|---|---|
| Volume of Water Ingested | Arithmetic mean: 25 mL h−1 | Normal | [22,23] | |
| Standard deviation: 5 mL h−1 | ||||
| Density of E. coli in Fecal Waste (Log10 range) | Human: 0.5–8.0 | Log10 range | Log-Uniform | [3] |
| Cattle/Domestic Animal: 5.0–6.7 | [3] | |||
| Wildlife: 2.0–9.5 | [24,25] | |||
| Density of Reference Pathogen in Fecal Waste (Log10 range) | Human (Norovirus): 3.0–7.5 | Log10 range | Log-Uniform | [1,3,4,33] |
| Cattle/Domestic Animal (Campylobacter): 1.2–7.3 | ||||
| Wildlife (Cryptosporidium): 2.3–3.8 | ||||
| Prevalence of Infection | Human: 100% | Percent ranges | Uniform | [3,4,5,26] |
| Cattle/Domestic Animal: 5–38% | ||||
| Wildlife: 5–50% | ||||
| Infectious Potential | Human: 100% | Percent ranges | Uniform | [3,5,20,27] |
| Cattle/Domestic Animal: 67–100% | ||||
| Wildlife: 0–33% | ||||
| Dose–Response Values 1 | Norovirus: α = 0.04, β = 0.055 | Beta-Binomial (ID50: 26 viral particles, 60% morbidity) 2 | Point Estimate | [31,34,35,36,37] |
| Campylobacter: α = 0.145, N50 = 7.59 | Beta-Poisson (ID50: 800 cfu, morbidity 28%)2 | |||
| Cryptosporidium: r = 0.09 | Exponential (ID50:8 oocysts, morbidity 50%) 2 | |||
| Concentration of E. coli in Field Data | LEO 2 (geometric mean: 163) | point estimates of the geometric mean (cfu 100 mL−1) | Point Estimate | [12] |
| Recreational Standard (geometric mean: 126) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gitter, A.; Mena, K.D.; Wagner, K.L.; Boellstorff, D.E.; Borel, K.E.; Gregory, L.F.; Gentry, T.J.; Karthikeyan, R. Human Health Risks Associated with Recreational Waters: Preliminary Approach of Integrating Quantitative Microbial Risk Assessment with Microbial Source Tracking. Water 2020, 12, 327. https://doi.org/10.3390/w12020327
Gitter A, Mena KD, Wagner KL, Boellstorff DE, Borel KE, Gregory LF, Gentry TJ, Karthikeyan R. Human Health Risks Associated with Recreational Waters: Preliminary Approach of Integrating Quantitative Microbial Risk Assessment with Microbial Source Tracking. Water. 2020; 12(2):327. https://doi.org/10.3390/w12020327
Chicago/Turabian StyleGitter, Anna, Kristina D. Mena, Kevin L. Wagner, Diane E. Boellstorff, Kyna E. Borel, Lucas F. Gregory, Terry J. Gentry, and Raghupathy Karthikeyan. 2020. "Human Health Risks Associated with Recreational Waters: Preliminary Approach of Integrating Quantitative Microbial Risk Assessment with Microbial Source Tracking" Water 12, no. 2: 327. https://doi.org/10.3390/w12020327