Why Do People Remain Attached to Unsafe Drinking Water Options? Quantitative Evidence from Southwestern Bangladesh

 ,
, 
Abstract
:1. Introduction
2. Variables Explaining Variation in User Attachment to Drinking Water Sources
3. Methods
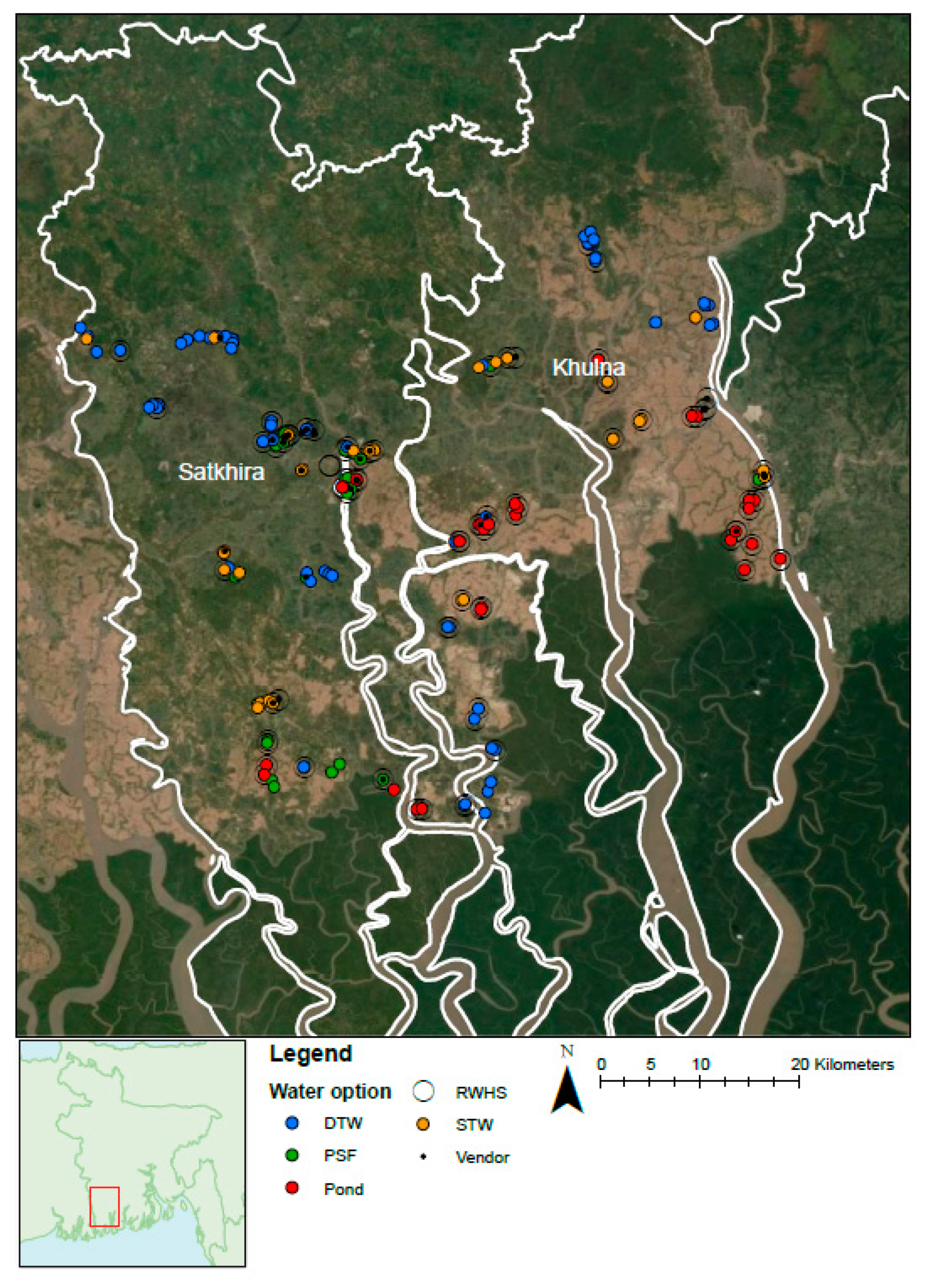
3.1. Sample Selection
3.2. Operationalisation of the Explanatory Variables
3.3. Data Analysis
4. Results
4.1. General Data
4.2. Explanatory Factors
4.3. Significant Differences Found for Explanatory Factors
5. Discussion
5.1. Improvement Strategies
5.1.1. Pond
5.1.2. Shallow Groundwater
5.2. Implementation Potential of the Investigated Alternatives
5.2.1. Rainwater Harvesting (RWH)
5.2.2. PSFs
5.2.3. DTWs
5.2.4. Vendor Water
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Compliance with Ethical Standards
Appendix A
- Very long (>60 min)
- Long (30–60 min)
- Medium (10–29 min)
- Short (5–9 min)
- Very short (<5 min)
- Strongly dislike
- Dislike
- Neutral
- Like
- Strongly like
- Very saline
- Saline
- Neutral
- Not saline/fresh
- Not saline at all/very fresh
- Expensive
- Cheap
- Free
- Very unhealthy
- Unhealthy
- Neutral
- Healthy
- Very healthy
- Large risk
- Some Risk
- Neutral
- No risk
- Strongly disapprove
- Disapprove
- Neutral
- Approve
- Strongly approve
- Few people/less than 10
- Intermediate amount of people/between 10 and 100
- Many people/more than 100
- Very unsure
- Unsure
- Neutral
- Sure
- Very sure
- Very unsure
- Unsure
- Neutral
- Sure
- Very sure
Appendix B

{kind=link}
| Unsafe Drinking Water Options | Safe Drinking Water Options | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Question | Pond, n = 30 | STW, n = 32 | PSF, n = 34 | Vendor, n = 30 | DTW, n = 70 | RWH, n = 66 | ||||||
| Mean | STD | Mean | STD | Mean | STD | Mean | STD | Mean | STD | Mean | STD | |
| Arsenic risk | 2.88 | 1.41 | 3.78 | 1.25 | 4.00 | 1.35 | 4.12 | 0.83 | 3.83 | 1.22 | 4.65 | 0.69 |
| Health | 2.03 | 1.13 | 3.00 | 1.02 | 3.50 | 0.99 | 3.66 | 0.86 | 3.80 | 1.04 | 4.42 | 0.70 |
| Collection time | 2.63 | 1.22 | 3.87 | 1.26 | 2.91 | 1.40 | 3.31 | 1.62 | 3.70 | 1.36 | 5.00 | 0.00 |
| Cost | 2.48 | 1.63 | 3.83 | 1.47 | 2.88 | 1.34 | 1.36 | 0.78 | 4.07 | 1.44 | 4.88 | 0.70 |
| Palatability | 2.63 | 0.85 | 3.69 | 0.90 | 3.85 | 0.74 | 3.80 | 0.85 | 4.04 | 0.86 | 4.64 | 0.57 |
| Neighbours’ opinion | 3.77 | 0.82 | 3.59 | 1.04 | 4.09 | 0.45 | 3.86 | 0.64 | 4.04 | 0.75 | 4.09 | 0.46 |
| Community size | 4.79 | 0.83 | 3.41 | 1.80 | 5 | 0 | 5 | 0 | 4.18 | 1.16 | 1.67 | 1.45 |
| Reliability | 3.73 | 1.48 | 4.16 | 0.99 | 3.27 | 1.35 | 3.27 | 1.43 | 4.07 | 1.06 | 2.95 | 1.32 |
| Habit | 3.27 | 1.31 | 4.23 | 0.82 | 3.91 | 0.97 | 3.39 | 1.29 | 4.36 | 0.73 | 4.57 | 0.83 |
References
- Hurlimann, A.; Dolnicar, S. Public acceptance and perceptions of alternative water sources: A comparative study in nine locations. Int. J. Water Resour. Dev. 2016, 32, 650–673. [Google Scholar] [CrossRef]
- Du Preez, M.; McGuigan, K.G.; Conroy, R.M. Solar disinfection of drinking water in the prevention of dysentery in South African children aged under 5 years: The role of participant motivation. Environ. Sci. Technol. 2010, 44, 8744–8749. [Google Scholar] [CrossRef] [PubMed]
- Mäusezahl, D.; Christen, A.; Pacheco, G.D.; Tellez, F.A.; Iriarte, M.; Zapata, M.E.; Cevallos, M.; Hattendorf, J.; Cattaneo, M.D.; Arnold, B.; et al. Solar drinking water disinfection (SODIS) to reduce childhood diarrhoea in rural Bolivia: A cluster-randomized, controlled trial. PLoS Med. 2009, 6, e1000125. [Google Scholar] [CrossRef] [PubMed]
- Peal, A.J.; Evans, B.E.; van der Voorden, C. Hygiene and Sanitation Software: An Overview of Approaches; Water Supply and Sanitation Collaborative Council: Geneva, Switzerland, 2010. [Google Scholar]
- Alam, M.; Sultana, M.; Nair, G.B.; Sack, R.B.; Sack, D.A.; Siddique, A.K.; Ali, A.; Huq, A.; Colwell, R.R. Toxigenic Vibrio cholerae in the Aquatic Environment of Mathbaria, Bangladesh. Appl. Environ. Microbiol. 2006, 72, 2849–2855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhuiyan, M.A.H.; Rakib, M.A.; Dampare, S.B.; Ganyaglo, S.; Suzuki, S. Surface water quality assessment in the central part of Bangladesh using multivariate analysis. KSCE J. Civ. Eng. 2011, 15, 995–1003. [Google Scholar] [CrossRef]
- Chowdhury, N.T. Water management in Bangladesh: An analytical review. Water Policy 2010, 12, 32. [Google Scholar] [CrossRef]
- Sharma, B.; Amarasinghe, U.; Xueliang, C.; de Condappa, D.; Shah, T.; Mukherji, A.; Bharati, L.; Ambili, G.; Qureshi, A.; Pant, D.; et al. The indus and the ganges: River basins under extreme pressure. Water Int. 2010, 35, 493–521. [Google Scholar] [CrossRef]
- Ayers, J.C.; Goodbred, S.; George, G.; Fry, D.; Benneyworth, L.; Hornberger, G.; Roy, K.; Karim, M.R.; Akter, F. Sources of salinity and arsenic in groundwater in southwest Bangladesh. Geochem. Trans. 2016, 17, 4. [Google Scholar] [CrossRef]
- Nickson, R.; McArthur, J.; Burgess, W.; Ahmed, K.M.; Ravenscroft, P.; Rahmanñ, M. Arsenic poisoning of Bangladesh groundwater. Nature 1998, 395, 338. [Google Scholar] [CrossRef]
- Harvey, C.F.; Swartz, C.H.; Badruzzaman, A.B.M.; Keon-Blute, N.; Yu, W.; Ali, M.A.; Jay, J.; Beckie, R.; Niedan, V.; Brabander, D.; et al. Arsenic Mobility and Groundwater Extraction in Bangladesh. Science 2002, 298, 1602–1606. [Google Scholar] [CrossRef] [Green Version]
- BGS; DPHE. Arsenic Contamination of Groundwater in Bangladesh; Kinniburgh, D.G., Smedley, P.L., Eds.; BGS Technical Report, WC/00/19; British Geological Survey: Keyworth, UK, 2001; Volume 2, ISBN 0852723849. [Google Scholar]
- Gaus, I.; Kinniburgh, D.G.; Talbot, J.C.; Webster, R. Geostatistical analysis of arsenic concentration in groundwater in Bangladesh using disjunctive kriging. Environ. Geol. 2003, 44, 939–948. [Google Scholar] [CrossRef] [Green Version]
- Naus, F.L.; Schot, P.; Groen, K.; Ahmed, K.M.; Griffioen, J. Groundwater salinity variation in Upazila Assasuni (southwestern Bangladesh), as steered by surface clay layer thickness, relative elevation and present-day land use. Hydrol. Earth Syst. Sci. 2019, 23, 1431–1451. [Google Scholar] [CrossRef] [Green Version]
- Naus, F.L.; Schot, P.; Ahmed, K.M.; Griffioen, J. Influence of landscape features on the large variation of shallow groundwater salinity in southwestern Bangladesh. J. Hydrol. X 2019, 5, 100043. [Google Scholar] [CrossRef]
- Worland, S.C.; Hornberger, G.M.; Goodbred, S.L. Source, transport, and evolution of saline groundwater in a shallow Holocene aquifer on the tidal deltaplain of southwest Bangladesh. Water Resour. Res. 2015, 51, 5791–5805. [Google Scholar] [CrossRef] [Green Version]
- Knappett, P.S.K.; Escamilla, V.; Layton, A.; McKay, L.D.; Emch, M.; Williams, D.E.; Huq, R.; Alam, J.; Farhana, L.; Mailloux, B.J.; et al. Impact of population and latrines on fecal contamination of ponds in rural Bangladesh. Sci. Total Environ. 2011, 409, 3174–3182. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, S.; Johnston, R.; Zheng, Y. Arsenic in tube well water in Bangladesh: Health and economic impacts and implications for arsenic mitigation. Bull. World Health Organ. 2012, 90, 839–846. [Google Scholar] [CrossRef]
- Khan, A.E.; Scheelbeek, P.F.D.; Shilpi, A.B.; Chan, Q.; Mojumder, S.K.; Rahman, A.; Haines, A.; Vineis, P. Salinity in Drinking Water and the Risk of (Pre)Eclampsia and Gestational Hypertension in Coastal Bangladesh: A Case-Control Study. PLoS ONE 2014, 9, e108715. [Google Scholar] [CrossRef] [Green Version]
- Sultana, S.; Ahmed, K.M.; Mahted-Ul-Alam, S.M.; Hasan, M.; Tuinhof, A.; Ghosh, S.K.; Rahman, M.S.; Ravenscroft, P.; Zheng, Y. Low-Cost Aquifer Storage and Recovery: Implications for Improving Drinking Water Access for Rural Communities in Coastal Bangladesh. J. Hydrol. Eng. 2014, 20, B5014007. [Google Scholar] [CrossRef]
- Harun, M.A.Y.A.; Kabir, G.M.M. Evaluating pond sand filter as sustainable drinking water supplier in the Southwest coastal region of Bangladesh. Appl. Water Sci. 2012, 3, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Kamruzzaman, A.K.M.; Ahmed, F. Study of Performence of Existing Pond Sand Filters in Different Parts of Bangladesh. In Sustainable Development of Water Resources, Water Supply and Environ-Mental Sanitation, Proceedings of the 32nd WEDC International Conference, Colombo, Sri Lanka, 13–17 November 2006; Loughborough University: Loughborough, UK, 2006; pp. 377–380. [Google Scholar]
- Kjellén, M.; McGranahan, G. Informal Water Vendors and the Urban Poor; International Institute for Environment and Development: London, UK, 2006; ISBN 978-1-84369-586-8. [Google Scholar]
- Despins, C.; Farahbakhsh, K.; Leidl, C. Assessment of rainwater quality from rainwater harvesting systems in Ontario, Canada. J. Water Supply Res. Technol. AQUA 2009, 58, 117–134. [Google Scholar] [CrossRef] [Green Version]
- Dobrowsky, P.H.; De Kwaadsteniet, M.; Cloete, T.E.; Khan, W. Distribution of Indigenous Bacterial Pathogens and Potential Pathogens Associated with Roof-Harvested Rainwater. Appl. Environ. Microbiol. 2014, 80, 2307–2316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabir, A.; Howard, G. Sustainability of arsenic mitigation in Bangladesh: Results of a functionality survey. Int. J. Environ. Health Res. 2007, 17, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Inauen, J.; Hossain, M.M.; Johnston, R.B.; Mosler, H.J. Acceptance and Use of Eight Arsenic-Safe Drinking Water Options in Bangladesh. PLoS ONE 2013, 8, e53640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosler, H.J.; Blöchliger, O.R.; Inauen, J. Personal, social, and situational factors influencing the consumption of drinking water from arsenic-safe deep tubewells in Bangladesh. J. Environ. Manag. 2010, 91, 1316–1323. [Google Scholar] [CrossRef] [Green Version]
- George, C.M.; Inauen, J.; Perin, J.; Tighe, J.; Hasan, K.; Zheng, Y. Behavioral Determinants of Switching to Arsenic-Safe Water Wells: An Analysis of a Randomized Controlled Trial of Health Education Interventions Coupled with Water Arsenic Testing. Health Educ. Behav. 2017, 44, 92–102. [Google Scholar] [CrossRef]
- Mosler, H. A systematic approach to behavior change interventions for the water and sanitation sector in developing countries: A conceptual model, a review, and a guideline. Int. J. Environ. Health Res. 2012, 22, 431–449. [Google Scholar] [CrossRef]
- Heri, S.; Mosler, H.J. Factors affecting the diffusion of solar water disinfection: A field study in Bolivia. Health Educ. Behav. 2008, 35, 541–560. [Google Scholar] [CrossRef]
- Graf, J.; Meierhofer, R.; Wegelin, M.; Mosler, H.J. Water disinfection and hygiene behaviour in an urban slum in Kenya: Impact on childhood diarrhoea and influence of beliefs. Int. J. Environ. Health Res. 2008, 18, 335–355. [Google Scholar] [CrossRef] [Green Version]
- Huber, A.C.; Bhend, S.; Mosler, H.J. Determinants of exclusive consumption of fluoride-free water: A cross-sectional household study in rural Ethiopia. J. Public Health 2012, 20, 269–278. [Google Scholar] [CrossRef]
- Matell, M.S.; Jacoby, J. Is there an optimal number of alternatives for Likert scale items? Study I: Reliability and validity. Educ. Psychol. Meas. 1971, 31, 657–674. [Google Scholar] [CrossRef]
- Kruskal, W.H.; Wallis, W.A. Use of Ranks in One-Criterion Variance Analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Dunn, O.J. Multiple Comparisons Using Rank Sums. Technometrics 1964, 6, 241–252. [Google Scholar] [CrossRef]
- Hasan, M.B.; Driessen, P.P.J.; Majumder, S.; Zoomers, A.; Van Laerhoven, F. Factors Affecting Consumption of Water from a Newly Introduced Safe Drinking Water System: The Case of Managed Aquifer Recharge (MAR) Systems in Bangladesh. Water 2019, 11, 2459. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.A.; Sakakibara, H.; Sekine, M.; Karim, M.R. Potable water scarcity: Options and issues in the coastal areas of Bangladesh. J. Water Health 2013, 11, 532–542. [Google Scholar] [CrossRef] [Green Version]
- Sirajul Islam, M.; Brooks, A.; Kabir, M.S.; Jahid, I.K.; Shafiqul Islam, M.; Goswami, D.; Nair, G.B.; Larson, C.; Yukiko, W.; Luby, S. Faecal contamination of drinking water sources of Dhaka city during the 2004 flood in Bangladesh and use of disinfectants for water treatment. J. Appl. Microbiol. 2007, 103, 80–87. [Google Scholar] [CrossRef]
- Faisal, I.M.; Kabir, M.R. An Analysis of Gender–Water Nexus in Rural Bangladesh. J. Dev. Soc. 2005, 21, 175–194. [Google Scholar] [CrossRef]
- Altherr, A.M.; Mosler, H.J.; Tobias, R.; Butera, F. Attitudinal and relational factors predicting the use of solar water disinfection: A field study in nicaragua. Health Educ. Behav. 2008, 35, 207–220. [Google Scholar] [CrossRef] [Green Version]
- Moser, S.; Mosler, H.J. Differences in influence patterns between groups predicting the adoption of a solar disinfection technology for drinking water in Bolivia. Soc. Sci. Med. 2008, 67, 497–504. [Google Scholar] [CrossRef]
- Opar, A.; Pfaff, A.; Seddique, A.A.; Ahmed, K.M.; Graziano, J.H.; van Geen, A. Responses of 6500 households to arsenic mitigation in Araihazar, Bangladesh. Health Place 2007, 13, 164–172. [Google Scholar] [CrossRef]
- Peters, C.N.; Baroud, H.; Hornberger, G.M. Multicriteria Decision Analysis of Drinking Water Source Selection in Southwestern Bangladesh. J. Water Resour. Plan. Manag. 2019, 145, 05019004. [Google Scholar] [CrossRef]
- Hossain, M.; Rahman, S.N.; Bhattacharya, P.; Jacks, G.; Saha, R.; Rahman, M. Sustainability of arsenic mitigation interventions-an evaluation of different alternative safe drinking water options provided in Matlab, an arsenic hot spot in Bangladesh. Front. Environ. Sci. 2015, 3, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Hoque, B.A.; Hoque, M.M.; Ahmed, T.; Islam, S.; Azad, A.K.; Ali, N.; Hossain, M.; Hossain, M.S. Demand-based water options for arsenic mitigation: An experience from rural Bangladesh. Public Health 2004, 118, 70–77. [Google Scholar] [CrossRef]

| Explanatory Factors | Definition | Interview Questions |
|---|---|---|
| Risk | ||
| Vulnerability | Risk of arsenic | How high or low do you think is the risk that you will develop arsenicosis? High risk = 1; Some risk = 2; Neutral = 3; No risk = 4 |
| Health risk | How healthy do you think your drinking water is? Very unhealthy = 1; Unhealthy = 2; Neutral = 3; Healthy = 4; Very healthy = 5 | |
| Attitudes | ||
| Instrumental beliefs | Collection Time | How long does it take in minutes to collect the water from the moment you leave the house until you come back (including walking, queuing, collecting)? Very short (<5 min) = 5; Short (5–9 min) = 4; medium (10–29 min) = 3; Long (30–60 min) = 2; Very long (>60 min) = 1 |
| Cost | How do you feel about the cost of your water? Expensive = 1; Cheap = 2; Free = 3 | |
| Affective beliefs | Palatability | How much do you like or dislike the taste of your drinking water? Strongly dislike = 1; Dislike = 2; Neutral = 3; Like = 4; Strongly like = 5 |
| Norms | ||
| Injunctive norm | Neighbours’ opinion | Do your neighbours approve or disapprove of your drinking water source? Strongly disapprove = 1; Disapprove = 2; Neutral = 3; Approve = 4; Strongly approve = 5 |
| Descriptive norm | Regular convention | How many people from your community get water from your drinking water source? Few people/less than 10 = 1; Intermediate amount of people/between 10 and 100 = 2; Many people/more than 100 = 3 |
| Reliability | ||
| Reliability | Will you be able to get water from your drinking water option in a month’s time? Very unsure = 1; Unsure = 2; Neutral = 3; Sure = 4; Very sure = 5 | |
| Habit | ||
| Habit | Do you use your drinking water option out of habit? Very unsure = 1; Unsure = 2; Neutral = 3; Sure = 4; Very sure = 5 |
| Option | No. of Completed Questionnaires | Percentage Sole Drinking Water Option | Multiple Drinking Water Options | Median Cost (BDT/L) | Average Cost (BDT/L) | Usage L/(Day, Person) |
|---|---|---|---|---|---|---|
| Pond | 30 | 7% | 93% | 0.006 | 0.335 | 3.1 |
| STW | 32 | 44% | 56% | 0 | 0.031 | 4.3 |
| DTW | 70 | 69% | 31% | 0 | 0.077 | 3.1 |
| RWH | 66 | 1% | 99% | 0 | 0 | 2.6 |
| PSF | 34 | 35% | 65% | 0.022 | 0.131 | 3.1 |
| Vendor | 30 | 7% | 93% | 0.833 | 0.975 | 2.5 |
| Unsafe Drinking Water Options | Safe Drinking Water Options | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Explanatory Factor | Pond, n = 30 | STW, n = 32 | PSF, n = 34 | Vendor, n = 30 | DTW, n = 70 | RWH, n = 66 | ||||||
| Mean | STD | Mean | STD | Mean | STD | Mean | STD | Mean | STD | Mean | STD | |
| Risk = | 2.28 | 1.06 | 3.28 | 0.98 | 3.69 | 0.95 | 3.87 | 0.69 | 3.89 | 0.95 | 4.47 | 0.63 |
| Attitude & | 2.59 | 0.66 | 3.81 | 0.71 | 3.21 | 0.82 | 2.86 | 0.73 | 3.95 | 0.76 | 4.81 | 0.33 |
| Norms ^ | 4.22 | 0.68 | 3.5 | 1.09 | 4.49 | 0.29 | 4.21 | 0.54 | 4.06 | 0.73 | 3.81 | 0.74 |
| Reliability # | 3.73 | 1.48 | 4.16 | 0.99 | 3.27 | 1.35 | 3.27 | 1.43 | 4.02 | 1.05 | 2.95 | 1.32 |
| Habit ~ | 3.27 | 1.31 | 4.23 | 0.82 | 3.91 | 0.97 | 3.39 | 1.29 | 4.3 | 0.76 | 4.57 | 0.83 |
| Explanatory Factor | Brackish STW | n = 13 | Fresh STW | n = 15 | Significance Dunn’s Test |
|---|---|---|---|---|---|
| Mean | Std | Mean | Std | ||
| Risk = | 3.19 | 1.03 | 3.34 | 0.97 | |
| Attitude & | 3.35 | 0.70 | 4.12 | 0.54 | * |
| Norms ^ | 3.62 | 0.87 | 3.42 | 1.23 | |
| Reliability # | 4.62 | 0.87 | 3.84 | 0.96 | + |
| Habit ~ | 4.42 | 1.00 | 4.11 | 0.68 |
| Drinking Water Options | Group1 | Group2 | Risk = | Attitude & | Norms ^ | Reliability # | Habit ~ |
|---|---|---|---|---|---|---|---|
| p-Value for Each Explanatory Factor | |||||||
| Unsafe | Pond | STW | * | + | |||
| Pond | PSF | * | |||||
| Pond | Vendor | * | |||||
| Pond | DTW | * | * | * | |||
| Pond | RWH | * | * | + | * | ||
| STW | PSF | * | |||||
| STW | Vendor | + | |||||
| STW | DTW | ||||||
| STW | RWH | * | * | + | |||
| Safe | PSF | Vendor | |||||
| PSF | DTW | * | |||||
| PSF | RWH | * | * | + | * | ||
| Vendor | DTW | * | * | ||||
| Vendor | RWH | * | * | * | |||
| DTW | RWH | * | * | + | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naus, F.L.; Burer, K.; van Laerhoven, F.; Griffioen, J.; Ahmed, K.M.; Schot, P. Why Do People Remain Attached to Unsafe Drinking Water Options? Quantitative Evidence from Southwestern Bangladesh. Water 2020, 12, 342. https://doi.org/10.3390/w12020342
Naus FL, Burer K, van Laerhoven F, Griffioen J, Ahmed KM, Schot P. Why Do People Remain Attached to Unsafe Drinking Water Options? Quantitative Evidence from Southwestern Bangladesh. Water. 2020; 12(2):342. https://doi.org/10.3390/w12020342
Chicago/Turabian StyleNaus, Floris Loys, Kennard Burer, Frank van Laerhoven, Jasper Griffioen, Kazi Matin Ahmed, and Paul Schot. 2020. "Why Do People Remain Attached to Unsafe Drinking Water Options? Quantitative Evidence from Southwestern Bangladesh" Water 12, no. 2: 342. https://doi.org/10.3390/w12020342