
Dementia and Parkinson’s Disease: Risk Factors for 30-Day Mortality in Nursing Home Residents with COVID-19
Abstract
Background:
The COVID-19 pandemic has led to high mortality rates in nursing homes (NHs) in Europe. For adequate risk management and good prognostications, it is essential to identify mortality risk factors.
Objective:
This study aimed to determine whether previously identified risk factors for 30-day mortality in Dutch NH residents with COVID-19 are unique to COVID-19.
Methods:
In this cohort study, we included 1,294 NH residents with COVID-19 (cases) and 17,999 NH residents without COVID-19 (controls, from the pre-COVID-19 period). We used descriptive statistics and Cox proportional hazard models to compare mortality rates in residents with and without COVID-19, categorized by risk factors.
Results:
Cases had a more than 18 times higher hazard of death within 30 days compared to controls (HR 18, 95%CI: 16–20). For residents with COVID-19, being male, having dementia, and having Parkinson’s disease (PD) were all associated with a higher 30-day mortality (HR 1.8 versus 1.3 versus 1.7). Being male was also associated with a higher mortality (HR 1.7) in the control group, whereas having dementia and PD were not. COVID-19 symptomatology was very similar for residents with and without dementia or PD, except for delirium and malaise which was more frequent in residents with dementia.
Conclusion:
Dementia and PD were significant additional risk factors for mortality in Dutch NH residents with COVID-19, whereas male gender was not unique to residents with COVID-19. The frailty of PD and dementia in NH residents with COVID-19 are relevant to consider in prognostication, communication, and care planning with residents and their families.
INTRODUCTION
The COVID-19 pandemic has resulted in high mortality rates in nursing homes (NHs) in Europe. Comparison of the same time-period showed an 81%to 315%increase in all-cause death rate in 2020 in different NHs across Europe [1–4]. In the Netherlands, the number of deaths per week in NHs increased with approximately 100%during the first months of the COVID-19 pandemic [5].
For adequate risk management and good prognostication, it is essential to identify factors specifically associated with high 30-day mortality in NH residents with COVID-19. In an earlier study among Dutch NH residents with confirmed COVID-19, we established that male sex, renal failure, dementia, and Parkinson’s disease (PD) were associated with a higher mortality rate [6]. Higher mortality rates in NH residents with dementia and PD were also observed in other studies [7–9]. In addition, frailty, chronic obstructive pulmonary disease or emphysema, and cardiovascular disease have been reported as risk factors for mortality in NH residents with COVID-19 [3, 10, 11].
In the abovementioned studies, mortality rates of NH residents with COVID-19 were compared to those of NH residents without COVID-19 (i.e., a negative reverse transcriptase polymerase chain reaction (RT-PCR) test) during the COVID-19 period. Due to the limited test capacity at the start of the pandemic, only residents with respiratory symptoms were tested. As a result, the control group consisted of residents that may have been at risk for mortality because of having influenza or another underlying cause of the respiratory symptoms. Since the sensitivity of the RT-PCR is limited [12], it is possible that a part of the control group had a false-negative test and therefore still had COVID-19. The present study attempts to advance current knowledge by comparing NH residents with COVID-19 to NH residents without COVID-19 from the pre-COVID-19 period, ensuring a control group without residents suffering from COVID-19 and with less selection bias (e.g., not only residents with symptoms).
We investigate whether our previously identified risk factors for 30-day mortality (i.e., male gender, kidney failure, dementia, and PD) in Dutch NH residents are unique to COVID-19, or whether these are risk factors for mortality among NH residents in general. In addition, we also compare patient characteristics and symptomatology of COVID-19 in Dutch NH residents with and without those risk factors to gain a better understanding of the impact of COVID-19 in these NH residents.
METHODS
We conducted a cohort study where Dutch NH residents with confirmed COVID-19 were compared with Dutch NH residents of the pre-COVID-19 era (i.e., without COVID-19). For both groups, data were derived from the electronic health record (EHR) Ysis. Ysis, managed by software developer Gerimedica, is the most widely used EHR in NHs in the Netherlands and covers over 61,000 out of a total of 115,000 NH residents.
Data collection and measures
Cases were defined as NH residents with COVID-19 confirmed by RT-PCR in the period between March 18 and May 31, 2020. For these residents, a standardized assessment form was completed by their physician as part of national COVID-19 registration policy. This form included data on the presence (yes/no) of fever, cough, shortness of breath, sore throat, and delirium/confusion/drowsiness. It also included oxygen saturation (normal versus decreased), body temperature, and an open question on presence of any other signs or symptoms. Age, sex, type of ward, date of death, and comorbidity (i.e., dementia (including mild cognitive impairment), chronic respiratory diseases, chronic cardiovascular disease, cerebrovascular diseases, diabetes mellitus, reduced kidney function, and PD (including parkinsonism) were derived from usual care data in the EHR [6].
COVID-19 test policy in the Netherlands, as defined by the Dutch Association of Elderly Care Physicians (Verenso), differed throughout the period of data collection due to initial scarcity of available test materials. Until March 26, 2020, it was advised to perform RT-PCR testing only in NH residents with at least two of the following symptoms: fever or feverish feeling, cough, and shortness of breath, and, only at wards without any proven cases of COVID-19 (at such wards clinically-suspected COVID-19 cases were considered COVID-19 patients). From March 26, 2020, onwards, it was advised to test NH residents with any possibly COVID-19 related symptoms at wards without any proven COVID-19 cases; from April 6, 2020, this advice became applicable also for residents at wards with COVID-19 cases.
For the control group, we extracted data from 17,999 randomly selected NH residents in the same period in which data for COVID-19 patients were collected, except one year earlier. This was the maximum number of controls that we could request within the data protection measures applied by the data processor. As in other studies using similar analyses [13, 14], a number of four or five controls per case were selected, we are confident that the size of the control group in our study was large enough to capture statistically significant and clinically relevant differences between the residents with COVID-19 and the controls. We extracted data on age, gender, type of ward, and comorbidities on April 1, 2019 and to calculate the 30-day mortality, we recorded the date of death between April 1, 2019 and May 1, 2019. To avoid duplicate cases, we ensured that NH residents with a confirmed COVID-19 in 2020 were not included in the 2019 dataset.
Outcome measure
Outcome measure in this study was 30-day mortality, in the COVID-19 group defined as mortality within 30 days after the COVID-19 suspicion, and in the non-COVID-19 group as mortality within 30 days after inclusion (i.e., April 1, 2019).
Ethics
The Medical Ethics Committee of the VU University Medical Centre reviewed and approved the study protocol.
Statistical analyses
For both groups, survival curves on 30 day-mortality were estimated based on the days between the date of COVID-19 suspicion (COVID-19 group) or inclusion (control group, i.e., April 1, 2019) and the date of death using Kaplan Meier curves. The association between age, gender, comorbidities, symptomatology, and mortality rate was analyzed in residents with COVID-19 and the controls using three Cox proportional hazard models: unadjusted (model 1); gender and age included (model 2); and gender, age, and comorbidities included (model 3). We investigated with effect modification analyses whether the effect of specific risk factors (i.e., being male, having dementia, having PD) on time to death was different for residents with and without COVID-19. In these analyses, the interaction between the group variable (COVID-19) and the risk factor was included in the model. Results are presented with 95%confidence intervals and all reported p values are two-sided.
Next, patient characteristics and symptomatology of COVID-19 patients with and without unique identified risk factors were analyzed descriptively. We used Mann-Whitney U test for non-parametric continuous variables and chi-square tests for categorical variables to compare demographic characteristics and symptomatology. To indicate the number of missing values, the N on which percentages were calculated, are reported.
All analyses were performed with the use of the SPSS statistical package, version 26.0 (IBM, IL, USA).
RESULTS
Residents’ characteristics
We included 1,294 cases and 17,999 controls. Residents had a mean age of 83 years (SD: 10), were predominately women (66%) and resided mostly on psychogeriatric wards (51%) (Table 1). Residents with COVID-19 were more likely to have dementia (64%versus 56%) and suffered more often from a reduced kidney function (19%versus 13%). Except for these differences, no important clinical differences were found between the characteristics of residents with COVID-19 and the controls without COVID-19.
Table 1
Residents’ characteristics
| Total | COVID-19 | Control | |
| (N = 19,293) | (N = 1,294) | (N = 17,999) | |
| Age: mean (SD) | 83 (10) | 84 (9) | 83 (10) |
| Women | 66% | 64% | 66% |
| Ward type | |||
| Psychogeriatric | 51% | 48% | 51% |
| Somatic | 24% | 18% | 25% |
| Rehabilitation/short term care | 18% | 18% | 18% |
| Other/Unknown | 7% | 17% | 6% |
| Comorbidity | (N = 19,170) | (N = 1,284) | (N = 17,886) |
| Dementia | 56% | 64% | 56% |
| Cardiovascular disease | 41% | 44% | 41% |
| Cerebrovascular disease | 35% | 35% | 35% |
| Diabetes Mellitus | 24% | 26% | 24% |
| Chronic respiratory disease | 16% | 17% | 16% |
| Reduced kidney function | 13% | 19% | 13% |
| Parkinson’s disease | 7% | 6% | 7% |
3.230-day mortality risk
We found that 42%(95%CI: 39–45%) of the residents with COVID-19 had died within 30 days after the COVID-19 suspicion, and 3.2%(95%CI: 3.0–3.4%) of the controls died within 30 days (Fig. 1A). Adjusted for age, sex, and comorbidity, residents with COVID-19 had an 18 times higher hazard of death compared to controls (HR 18, 95%CI: 16–20) (Table 2).
Fig. 1
Kaplan-Meier estimates of survival in nursing home residents with confirmed and without COVID-19, overall (A), categorized based on gender (B), categorized based on presence of dementia (C), and categorized based on presence of Parkinson’s disease (D).
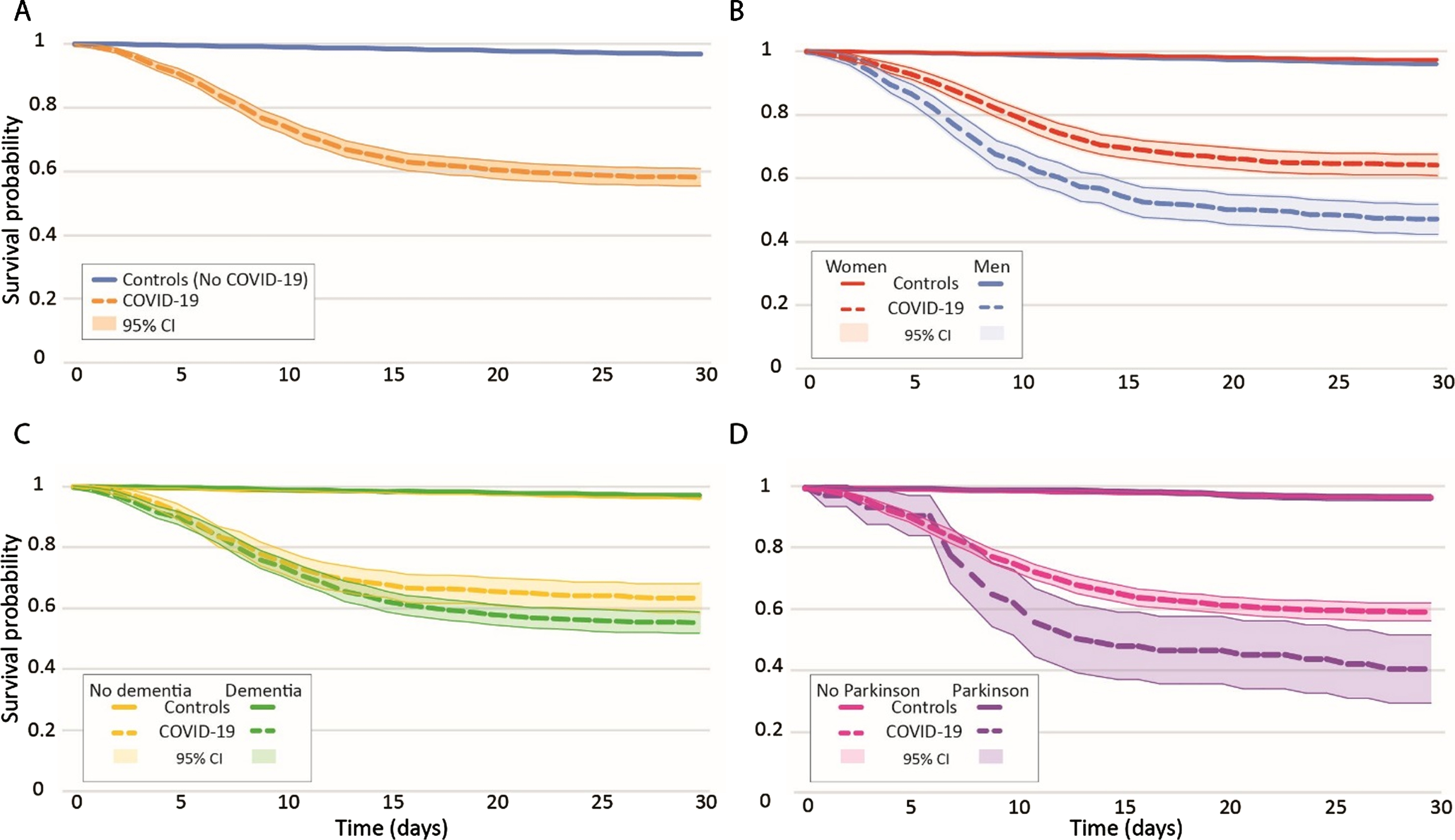
Table 2
Cox proportional Hazard model for 30-day mortality in nursing home residents with and without COVID-19
| Model 1: unadjusted | Model 2: adjusted for gender and age | Model 3: adjusted for gender, age, and comorbidity | ||||
| HR (95%CI) | p | HR (95%CI) | p | HR (95%CI) | p | |
| CONTROL | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | |||
| COVID-19 | 17.97 (15.94–20.26)* | <0.001* | 17.73 (15.72–19.99)* | <0.001* | 17.72 (15.70–20.01)* | <0.001* |
3.3Risk factors for 30-day mortality
We found that being male (adjusted HR 1.82, 95%CI: 1.52–2.18), having a dementia diagnosis (adjusted HR 1.28, 95%CI: 1.06–1.54), and suffering from PD (adjusted HR 1.67, 95%CI: 1.22–2.28) were all associated with a higher mortality within 30 days in residents with COVID-19 (Table 3). Kidney failure was no longer associated with higher mortality within 30 days (HR 1.22, 95%CI: 0.99–1.51). We performed effect modification analyses to explore whether the impact of these risk factors on time to death differed between residents with and without COVID-19. We found not a significant interaction for COVID-19 and gender. Being male was also a risk factor for mortality within 30 days in residents without COVID-19 (adjusted HR 1.68, 95%CI: 1.41–1.99). We did find a significant interaction for COVID-19 and dementia and for COVID-19 and PD. In residents without COVID-19, dementia, and PD were not risk factors for mortality within 30 days (adjusted HR 0.89, 95%CI: 0.75–1.06 versus adjusted HR 1.01, 95%CI: 0.73–1.39).
Table 3
Cox proportional Hazard model for risk factors for 30-day mortality in nursing home residents with (N = 1,294) and without COVID-19 (N = 17,999)
| Model 1: unadjusted | Model 2: adjusted for gender and age | Model 3: adjusted for gender, age, and comorbidity | |||||||
| COVID-19 HR (95%CI) | CONTROL HR (95%CI) | p interaction term | COVID-19 HR (95%CI) | CONTROL HR (95%CI) | p Interaction term | COVID-19 HR | CONTROL HR | p Interaction term | |
| (COVID-19*risk | (COVID-19*risk factor) | (95%CI) | (95%CI) | (COVID-19*risk factor) | |||||
| Male gender | 1.70 (1.43–2.03)* | 1.48 (1.25–1.75)* | 0.178 | 1.86 (1.56–2.23)* | 1.70 (1.43–2.02)* | 0.249 | 1.82 (1.52–2.18)* | 1.68 (1.41–1.99)* | 0.236 |
| Dementia | 1.25 (1.04–1.51)* | 0.96 (0.81–1.13) | 0.040* | 1,25 (1.04–1,52)* | 0.89 (0.75–1.05) | 0.015* | 1.28 (1.06–1.54)* | 0.89 (0.75–1.06) | 0.012* |
| PD | 1.64 (1.21–2.22)* | 1.03 (0.75–1.42) | 0.032* | 1.62 (1.19–2.21)* | 1.01 (0.73–1.40) | 0.021* | 1.67 (1.22–2.28)* | 1.01 (0.73–1.39) | 0.020* |
Characteristics of and COVID-19 symptomatology in high-risk residents
Dementia and PD were significant additional risk factors for mortality in NH residents with COVID-19. We found that 45%(95%CI: 41–48%) of the residents with dementia and COVID-19 had died within 30 days after the COVID-19 suspicion. Residents with COVID-19 and dementia (n = 816, 63%) were older than residents with COVID-19 and without dementia (85 versus 83 years) and resided more often on psychogeriatric wards (65%versus 19%) (Table 4). ‘Typical’ COVID-19 signs and symptoms did not differ between residents with and without dementia. However, signs of delirium (31%versus 24%) and malaise (6%versus 3%) were reported more commonly in residents with dementia, while diarrhea was reported more frequently in residents without dementia (4%versus 7%). There were no differences in comorbidity between residents with and without dementia who had COVID-19.
Table 4
Characteristics of and symptomatology in nursing home residents with COVID-19 (n = 1,294) and dementia or Parkinson’s disease (PD)
| Dementia (N = 816) | No dementia (N = 468) | p (Dementia versus no dementia) | PD (N = 77) | No PD (N = 1,207) | p (PD versus no PD) | |
| Age: mean (SD) | 85 (7) | 83 (10) | 0.013 | 81 (7) | 85 (9) | 0.000 |
| Women | 66% | 61% | 0.064 | 46% | 65% | 0.000 |
| Ward type | 0.000 | 0.001 | ||||
| Psychogeriatric | 65% | 19% | 42% | 49% | ||
| Somatic | 8% | 34% | 35% | 17% | ||
| Rehabilitation/short term care | 10% | 30% | 14% | 18% | ||
| Other/Unknown | 16% | 17% | 9% | 17% | ||
| Comorbidity | (N = 816) | (N = 468) | (N = 77) | (N = 1,207) | ||
| Dementia | – | – | – | 61% | 64% | 0.637 |
| Cardiovascular disease | 42% | 47% | 0.117 | 42% | 44% | 0.666 |
| Cerebrovascular disease | 34% | 36% | 0.708 | 29% | 35% | 0.236 |
| Diabetes Mellitus | 25% | 27% | 0.469 | 26% | 26% | 0.929 |
| Chronic respiratory disease | 15% | 19% | 0.081 | 10% | 17% | 0.120 |
| Reduced kidney function | 19% | 18% | 0.836 | 9% | 19% | 0.029 |
| Parkinson’s disease | 6% | 6% | 0.637 | – | – | – |
| Typical symptoms | ||||||
| Cough | 62% (477/773) | 62% (270/437) | 0.979 | 62% (41/66) | 62% (706/1,144) | 0.947 |
| Shortness of breath | 27% (202/745) | 32% (138/430) | 0.070 | 28% (19/69) | 29% (321/1,106) | 0.792 |
| Fever | 62% (483/784) | 64% (289/451) | 0.387 | 65% (47/72) | 62% (725/1,163) | 0.617 |
| Atypical symptoms | ||||||
| Sore throat | 9% (45/502) | 11% (36/323) | 0.304 | 9% (4/45) | 10% (77/780) | 0.829 |
| Delirium/confusion/drowsiness | 31% (219/704) | 24% (94/394) | 0.011* | 35% (23/66) | 28% (290/1,032) | 0.239 |
| Other symptoms* | ||||||
| Fatigue | 7% (60/816) | 5% (25/468) | 0.166 | 5% (4/77) | 7% (81/1,207) | 0.603 |
| Diarrhea | 4% (32/816) | 7% (33/468) | 0.013* | 3% (2/77) | 5% (63/1,207) | 0.308 |
| Malaise | 6% (47/816) | 3% (14/468) | 0.025* | 3% (2/77) | 5% (59/1,207) | 0.359 |
| Rhinorrhea | 3% (23/816) | 4% (17/468) | 0.415 | 0% (0/77) | 3% (40/1,207) | 0.104 |
| Nausea/vomiting | 3% (24/816) | 4% (19/468) | 0.280 | 3% (2/77) | 3% (41/1,207) | 0.705 |
| Common cold | 3% (27/816) | 3% (13/468) | 0.603 | 0% (0/77) | 3% (40/1,207) | 0.104 |
| Decreased oxygen saturation | 44% (238/543) | 47% (156/329) | 0.302 | 40% (23/58) | 46% (371/814) | 0.381 |
| Temperature | 0.443 | 0.088 | ||||
| <36.5°C | 4% (29/669) | 5% (19/374) | 8% (5/60) | 4% (43/983) | ||
| 36.5 –37.5°C | 18% (118/669) | 15% (55/374) | 17% (10/60) | 17% (163/983) | ||
| 37.5 –38.0°C | 18% (120/669) | 16% (60/374) | 7% (4/60) | 18% (176/983) | ||
| >38.0°C | 60% (402/669) | 64% (240/374) | 68% (41/60) | 61% (601/983) | ||
For residents with PD with COVID-19, we found that 60%(95%CI: 48–71%) had died. Residents with COVID-19 and PD (n = 77, 6%; disease duration (M = 7, SD = 5.18, n = 63)) were younger (81 versus 85 years), were more often male (54%versus 35%), and resided more often on a somatic ward (35%versus 17%) than residents with COVID-19 without PD (Table 4). COVID-19 symptomatology did not differ significantly between residents with PD and residents without PD. Residents with COVID-19 and PD suffered less often from kidney failure in comparison with residents without PD (9%versus 19%).
Effect of symptomatology on mortality
Fever, shortness of breath, delirium/confusion/drowsiness, and decreased oxygen were all associated with a higher mortality in NH residents with COVID-19 (HR 1.79, 95%CI: 1.47–2.18 versus HR 1.60, 95%CI: 1.32–1.94 versus HR 1.56, 95%CI: 1.28–1.90 versus HR 1.80, 95%CI: 1.46–2.23) (Table 5). Cough was not (HR 1.05, 95%CI: 0.87–1.26).
Table 5
Cox proportional Hazard model for symptomatology and 30-day mortality in nursing home residents with COVID-19 (N = 1,294)
| Model 1: unadjusted | Model 2: adjusted for gender and age | Model 3: adjusted for gender, age, and comorbidity | |
| HR (95%CI) | HR (95%CI) | HR (95%CI) | |
| Fever | 1.72 (1.42–2.09)* | 1.76 (1.45–2.15)* | 1.79 (1.47–2.18)* |
| Cough | 1.05 (0.87–1.26) | 1.05 (0.88–1.27) | 1.05 (0.87–1.26) |
| Shortness of breath | 1.66 (1.38–2.00)* | 1.56 (1.30–1.89)* | 1.60 (1.32–1.94)* |
| Delirium/confusion /drowsiness | 1.64 (1.35–2.00)* | 1.56 (1.28–1.90)* | 1.56 (1.28–1.90)* |
| Decreased oxygen saturation | 1.82 (1.47–2.24)* | 1.77 (1.43–2.18)* | 1.80 (1.46–2.23)* |
DISCUSSION
Thirty-day-mortality risk in Dutch NH residents with COVID-19 was 18 times higher than in a comparable group of NH residents without COVID-19. In residents with COVID-19, risk factors for 30-day mortality include male sex, dementia, and PD. Being male is not a 30-day mortality risk factor specific to COVID-19 in Dutch NH residents, leaving dementia and PD as risk factors unique to COVID-19.
Many studies, among which studies conducted in NHs, show that male sex is a risk factor for 30-day mortality of COVID-19 [3, 15]. To our best knowledge, we are the first to show that male sex is not a mortality risk factor specific to COVID-19 in NH residents, but that male sex is an independent risk factor for 30-day mortality in NH residents. This is in line with earlier studies that found an association between male sex and a lower survival rate after NH admission [16, 17]. Yet, given this a priori higher mortality risk combined with the high 30-day mortality risk of COVID-19, a COVID-19 diagnosis in male residents should be considered to be accompanied by a bad prognosis regarding 30-day mortality risk.
In our study, 45%of the residents with both COVID-19 and dementia died. This corresponds with the 42%mortality rate that was found in a study in patients of a tertiary hospital with Alzheimer’s disease or frontotemporal dementia [7], which were probably in a less severe stage compared with dementia patients in our study as 45%of them had very mild or mild dementia. We found that residents with COVID-19 and dementia had a 1.3 times higher hazard to die earlier than residents with COVID-19 without dementia. A meta-analysis showed that people with dementia and COVID-19 have a 2.6 times greater risk of mortality compared to COVID-19 patients without dementia [18]. Possible explanations that were given by the authors: 1) people with dementia are older and have more comorbidity, and 2) the APOE4 genotype, the major genetic risk factor for Alzheimer’s disease, is associated with more severe COVID-19 infection. The first explanation cannot be supported by our data, as we adjusted for age and we did not find any differences in comorbidity between residents with and without dementia. Regarding the second explanation, we do not have information on dementia subtypes nor the presence of the APOE4 genotype in the residents. Another explanation could be the high occurrence of delirium in patients with dementia. In our study residents with dementia more often had a delirium/confusion/drowsiness than residents without dementia (31%versus 24%). It is well known that a delirium is associated with higher mortality rates [19] and also in our study we observed a higher mortality rate for residents with COVID-19 and a delirium/confusion/drowsiness than for residents with COVID-19 without these symptoms (HR 1.6).
We established that residents with PD and COVID-19 have a strong increased risk of death, namely 60%, compared to COVID-19 positive residents without PD. This is a higher mortality rate than found in another study [9]. However, this study was done in a tertiary university hospital in a less vulnerable population. These PD patients were younger (76 versus 81 years) and had fewer comorbidities, for example 36%suffered from dementia, while 61%of the PD residents in our sample had dementia. It is possible that the high dementia rate in our PD population biased our results. However, duration of PD has also been described as risk factor for mortality in patients with COVID-19 and PD [8, 9]. Considering that duration of PD is an important indicator for both institutionalization and developing dementia, we might conclude, at least, that our NH residents with PD with a mean duration of 7 years were highly vulnerable and less likely to survive a COVID-19 infection.
Furthermore, previous studies suggested that a COVID-19 infection among PD patients may be accompanied by worsening of motor- and non-motor symptoms, due to a strong representation of ACE-2 receptors on dopamine receptors [20, 21]. This may also explain the relatively high mortality risk in this patient group. For instance, worsening of dysphagia may result in reduces fluid intake and dehydration, or aspiration followed by a pneumonia superinfection [9, 22]. In our study, we observed no differences in COVID-19 symptomatology between PD and non-PD residents; however, we did not register whether residents developed a pneumonia or pneumonia superinfection. Further research is needed to test these hypotheses on the effect of pneumonia and motor- and non-motor symptoms on mortality in NH residents with PD and COVID-19.
Strengths and limitations
Strengths of our study are the large number of cases included and the use of a control group from the pre-COVID-19 era. Our study has also limitations. First, we should discuss the probability of enrollment bias. Our registration was based on COVID-19 suspicion; therefore, our sample might show an overrepresentation of residents with typical signs and symptoms. Further, in the beginning of the pandemic, test materials were scarce, so from the start of our registration (March 18, 2020) until April 6, 2020 the advice was to test only symptomatic residents by RT-PCR, therefore, residents with an asymptomatic or paucisymptomatic course might have been missed in the registration. This enrollment bias may have resulted in an overestimation of mortality rates among residents with COVID-19, because COVID-19 residents with less severe or without any signs and symptoms were underrepresented. Second, for the same reason, we were not fully able to examine the occurrence of asymptomatic presentation of COVID-19 in residents with dementia and PD. Lastly, we were not able to correct mortality rates for factors such as medication use or acute illness such as influenza since we had no data about these factors.
CONCLUSION
Dutch NH residents with COVID-19 have an 18 times greater risk of death within 30 days compared to controls. Dementia and PD were significant additional risk factors for mortality in residents with COVID-19. Male sex was also an increased risk factor for mortality in residents with COVID-19, but this was not significantly higher than in the control group and thus is not unique to COVID-19.
Our findings highlight the importance of COVID-19 infection prevention in NHs and providing enough healthcare resources to implement such preventive strategies especially for institutionalized patients with PD and/or dementia, thereby also taking into account the potential negative consequences of preventive COVID-19 measures for quality of life in these subgroups.
Finally, our findings stress the frailty of PD and dementia in NH residents with COVID-19 and are relevant to consider in prognostication, communication and care planning with residents and their families.
ACKNOWLEDGMENTS
We thank the facility residents, the physicians who work in the long-term care facilities for their time to fill in the COVID-19 registration, and their ongoing efforts to provide care in the face of these and the staff of Gerimedica for their support.
This work was supported by the Dutch Ministry of Health, Welfare and Sport.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-0319r2).
REFERENCES
[1] | Cusack DA ((2020) ) COVID-19 pandemic: Coroner’s database of death inquiries with clinical epidemiology and total and excess mortality analyses in the District of Kildare March to June 2020. J Forensic Leg Med 76: , 102072. |
[2] | Mas Romero M , Avendaño Céspedes A , Tabernero Sahuquillo MT , Cortés Zamora EB , Gómez Ballesteros C , Sánchez-Flor Alfaro V , López Bru R , López Utiel M , Celaya Cifuentes S , Peña Longobardo LM , Murillo Romero A , Plaza Carmona L , Gil García B , Pérez Fernández-Rius A , Alcantud Córcoles R , Roldán García B , Romero Rizos L , Sánchez Jurado PM , León Ortiz M , Atienzar Núñez P , Noguerón García A , Ruiz García MF , García Molina R , Estrella Cazalla JD , Oliva Moreno J , Abizanda P ((2020) ) COVID-19 outbreak in long-term care facilities from Spain. Many lessons to learn. PLoS One 15: , e0241030. |
[3] | Graham NS , Junghans C , Downes R , Sendall C , Lai H , McKirdy A , Elliott P , Howard R , Wingfield D , Priestman M , Ciechonska M , Cameron L , Storch M , Crone M , Freemont P , Randell P , McLaren R , Lang N , Ladhani S , Sanderson F , Sharp DJ (2020) SARS-CoV-2 infection, clinical features and outcome of COVID-19 in United Kingdom nursing homes. medRxiv, 2020.2005.2019.20105460. |
[4] | Kennelly SP , Dyer AH , Noonan C , Martin R , Kennelly SM , Martin A , O’Neill D , Fallon A ((2020) ) Asymptomatic carriage rates and case-fatality of SARS-CoV-2 infection in residents and staff in Irish nursing homes. Age Ageing 50: , 49–54. |
[5] | RIVM, Excess mortality caused by novel coronavirus (Covid-19), –https://www.rivm.nl/node/155011. |
[6] | Rutten JJS , van Loon AM , van Kooten J , van Buul LW , Joling KJ , Smalbrugge M , Hertogh CMPM ((2020) ) Clinical suspicion of COVID-19 in nursing home residents: Symptoms and mortality risk factors. J Am Med Dir Assoc 21: , 1791–1797.e1. |
[7] | Matias-Guiu JA , Pytel V , Matías-Guiu J ((2020) ) Death rate due to COVID-19 in Alzheimer’s disease and frontotemporal dementia. J Alzheimers Dis 78: , 537–541. |
[8] | Fasano A , Elia AE , Dallocchio C , Canesi M , Alimonti D , Sorbera C , Alonso-Canovas A , Pezzoli G ((2020) ) Predictors of COVID-19 outcome in Parkinson’s disease. Parkinsonism Relat Disord 78: , 134–137. |
[9] | Sainz-Amo R , Baena-Álvarez B , Pareés I , Sánchez-Díez G , Pérez-Torre P , López-Sendón JL , Fanjul-Arbos S , Monreal E , Corral-Corral I , García-Barragán N , Martínez-Castrillo JC , Fasano A , Alonso-Cánovas A ((2021) ) COVID-19 in Parkinson’s disease: What holds the key? J Neurol 268: , 2666–2670. |
[10] | Shi SM , Bakaev I , Chen H , Travison TG , Berry SD ((2020) ) Risk factors, presentation, and course of coronavirus disease 2019 in a large, academic long-term care facility. J Am Med Dir Assoc 21: , 1378–1383.e1371. |
[11] | Tang O , Bigelow BF , Sheikh F , Peters M , Zenilman JM , Bennett R , Katz MJ ((2020) ) Outcomes of nursing home COVID-19 patients by initial symptoms and comorbidity: Results of universal testing of 1970 residents. J Am Med Dir Assoc 21: , 1767–1773.e1761. |
[12] | Watson J , Whiting PF , Brush JE ((2020) ) Interpreting a covid-19 test result. BMJ 369: , m1808. |
[13] | Joling KJ , Janssen O , Francke AL , Verheij RA , Lissenberg-Witte BI , Visser P , van Hout HPJ ((2020) ) Time from diagnosis to institutionalization and death in people with dementia. Alzheimers Dement 16: , 662–671. |
[14] | Rait G , Walters K , Bottomley C , Petersen I , Iliffe S , Nazareth I ((2020) ) Survival of people with clinical diagnosis of dementia in primary care: Cohort study. BMJ 341: , c3584. |
[15] | Chidambaram V , Tun NL , Haque WZ , Majella MG , Sivakumar RK , Kumar A , Hsu AT , Ishak IA , Nur AA , Ayeh SK , Salia EL , Zil EAA , Saeed MA , Sarena APB , Seth B , Ahmadzada M , Haque EF , Neupane P , Wang KH , Pu TM , Ali SMH , Arshad MA , Wang L , Baksh S , Karakousis PC , Galiatsatos P ((2020) ) Factors associated with disease severity and mortality among patients with COVID-19: A systematic review and meta-analysis. PLoS One 15: , e0241541. |
[16] | Reilev M , Lundby C , Jensen J , Larsen SP , Hoffmann H , Pottegård A ((2019) ) Morbidity and mortality among older people admitted to nursing home. Age Ageing 49: , 67–73. |
[17] | Hjaltadóttir I , Hallberg IR , Ekwall AK , Nyberg P ((2011) ) Predicting mortality of residents at admission to nursing home: A longitudinal cohort study. BMC Health Serv Res 11: , 86. |
[18] | Hariyanto TI , Putri C , Situmeang RFV , Kurniawan A ((2021) ) Dementia is a predictor for mortality outcome from coronavirus disease 2019 (COVID-19) infection. Eur Arch Psychiatry Clin Neurosci 271: , 393–395. |
[19] | Inouye SK ((2006) ) Delirium in older persons. N Engl J Med 354: , 1157–1165. |
[20] | Palermo G , Tommasini L , Baldacci F , Del Prete E , Siciliano G , Ceravolo R ((2020) ) Impact of coronavirus disease 2019 pandemic on cognition in Parkinson’s disease. Mov Disord 35: , 1717–1718. |
[21] | Cilia R , Bonvegna S , Straccia G , Andreasi NG , Elia AE , Romito LM , Devigili G , Cereda E , Eleopra R ((2020) ) Effects of COVID-19 on Parkinson’s disease clinical features: A community-based case-control study. Mov Disord 35: , 1287–1292. |
[22] | Antonini A , Leta V , Teo J , Chaudhuri KR ((2020) ) Outcome of Parkinson’s disease patients affected by COVID-19. Mov Disord 35: , 905–908. |

